

Stoyan R. Vezenkov, Pavlin P. Petrov and Violeta R. Manolova
Center for applied neuroscience Vezenkov, BG-1582 Sofia, e-mail: info@vezenkov.com
For citation: Vezenkov S.R., Petrov P.P., Manolova V.R. (2026) Screen Interaction, Not Screen Time: Multidimensional Framework, Global Policy Evidence, and Clinical Recommendations for Children with Screen Addiction and Screen Trauma. Nootism 2(2), 17-63, https://doi.org/10.64441/nootism.2.2.2
Abstract
Background. Children's digital exposure has triggered an unprecedented regulatory response: UNESCO reports 114 education systems with national mobile-phone restrictions as of March 2026, and multiple jurisdictions have enacted age-based social media prohibitions, early-childhood institutional bans, and platform-design obligations. Yet the dominant policy metric – aggregate screen-time duration – fails to capture the determinants of developmental risk. Adherence to current guidelines is consistently low (24.7% of families with children under two meet the zero-screen recommendation), and high-quality causal evidence on policy effects remains sparse.
Aims. We (i) propose screen interaction as the appropriate unit of analysis; (ii) operationalize the neurophysiologically grounded distinction between euthymic screen time (EST) – task-directed, design-bounded, adult-scaffolded engagement that preserves autonomic stability and cortical alertness – and hedonic screen time (HST) – pleasure- or state-shift-oriented, algorithmically served, architecturally engineered for compulsive use, and characterized by autonomic dominance and reduced cortical activation; (iii) map the international policy landscape to May 2026 across six regulatory models; (iv) review implementation evidence; and (v) introduce population-differentiated recommendations.
Methods. Narrative review and policy mapping through May 10, 2026, integrating peer-reviewed research, primary government and intergovernmental sources, and legal databases. Empirical claims are graded A (causal/quasi-experimental) through E (legal/media source).
Results – Conceptual. Screen interaction is defined by eight analytic dimensions (content type, device affordances, interactivity, social context, time of day, motivational purpose, design architecture, and the child's regulatory state), of which five have the strongest empirical support. Identical aggregate hours produce divergent outcomes depending on these dimensions, making duration a poor predictor of developmental risk.
Results – Policy. Six regulatory models are identified: A – school device restrictions (subtypes A1–A5, including A5 for school-issued devices and classroom screen-time caps); B – social media age restrictions; C – platform design regulation; D – early-childhood institutional prohibition; E – time-of-day regulation; F – clinical detection and health-system integration. Single-axis policies reliably reduce exposure within the regulated context but rarely reduce total daily exposure (SMART Schools, n=1,227; Reynolds, Ireland). Norway provides the strongest causal evidence (reduced mental-health utilization in girls; improved GPA in low-SES students). The implementation gap is severe: only 8.5% of French collèges had implemented the 2025 storage requirement at term start.
Clinical contribution. A clinically distinct subgroup develops a screen-trauma phenotype characterized by compulsive sensory seeking, withdrawal on device removal, collapse of joint attention, ASD-like or ADHD-like presentations, pathological screen-induced reflexes (SIPVR, SIPECR), and qEEG/HRV signatures of cortical splitting and autonomic dysregulation. For these children, generic time-limit guidance does not apply; a sequential clinical pathway (Nootism: containment → developmental-anchor resolution → sensory restart → reconnection → maintenance), with parallel parental therapeutic work, is required. Reversibility of ASD-like presentations after comprehensive therapy is documented in clinical cohorts; independent prospective validation is the principal research priority.
Conclusion. Existing policies are necessary but insufficient. Effective protection requires coordinated multi-axis regulation across school access, platform design, early-childhood institutional exposure, family behavior, and clinical pathways for affected children, with platform design regulation – addressing the autoplay, infinite-scroll, and variable-reward architectures that drive compulsive use – as the priority regulatory direction.
Keywords: screen interaction; screen time; screen addiction; screen trauma; hedonic screen time; euthymic screen time; reversed development; SIPVR; SIPECR; Nootism; six-model policy typology; digital policy; children; neurodevelopment; qEEG; HRV; social media restriction; school phone ban; platform design regulation
- Introduction
1.1 Current Context
Something has measurably shifted in the developmental landscape of childhood. Over the past fifteen years, clinicians, educators, and parents across high-income and middle-income countries have observed a convergence of trends: rising rates of anxiety, depression, and social disconnection among young people; a growing number of children presenting with features resembling autism spectrum disorder (ASD-like), attention deficit hyperactivity disorder (ADHD-like), and oppositional defiant disorder (ODD-like); and a steady decline in academic performance that preceded the COVID-19 pandemic by more than a decade (Braghieri et al., 2022; Haidt, 2024) [Grade B–C].
These trends have coincided with the mass adoption of smartphones, social media, and algorithmically served digital content. Facebook launched in 2004, the iPhone in 2007, and the steepest deterioration in adolescent mental health indicators began in the early 2010s, when social media reached saturation among young people (Haidt, 2024). Although these historical correlations do not by themselves establish causation, they have prompted an unprecedented policy response and a rapidly growing research literature on the developmental effects of digital exposure. The preceding version of this article documented these correlations and compiled the international policy responses that had emerged through mid-2025 (Petrov, Dimova, et al., 2025); the present article builds on that foundation, revises it conceptually, and extends it with implementation evidence and a differentiated clinical framework.
The OECD (2025) reports that adolescents in member countries spend, on average, more than four hours per day on digital devices outside school, with the steepest increases concentrated in the 10–15 age band [Grade E]. Centers for Disease Control and Prevention (Zablotsky et al., 2024) data indicate that approximately half of U.S. teenagers aged 12–17 report four or more hours of daily non-school screen use; among this group, 27.1% meet criteria for anxiety symptoms and 25.9% for depression symptoms [Grade C]. A systematic review and meta-analysis in JAMA Pediatrics drawing on 95 samples and 89,163 children found that only 24.7% of children under two years met the zero-screen recommendation, and only 35.6% of children aged two to five met the one-hour daily limit (McArthur et al., 2022) [Grade B] — establishing not only that exposure is high, but that existing guidelines are widely disregarded.
The developmental implications are no longer confined to behavioral observation. A growing body of psychophysiological and neurophysiological evidence associates early and intensive screen exposure with disruptions in autonomic regulation, attachment formation, language acquisition, and cortical organization (Hutton et al., 2020; Law et al., 2023a; Vezenkov & Manolova, 2026) [Grade C–D]. Healthy development depends on embodied, dyadic interaction – eye contact, vocal prosody, touch, and shared physical presence – which sustain the ventral vagal social engagement system (Porges, 2007, 2021, 2025) and activate the hormonal substrates of bonding: oxytocin and vasopressin release is contingent on direct social contact, not on screen-mediated approximations (Atzil et al., 2018; Eckstein et al., 2020) [Grade B]. Screen-based interaction can reduce or displace these inputs, particularly when it replaces embodied caregiver–child interaction during sensitive developmental windows (Carozza & Leong, 2021; Ilyka et al., 2021).
The developmental primacy of dyadic human exchange has been demonstrated most vividly by Tronick's Still Face Experiment (Tronick, 2007), in which a caregiver's sudden emotional non-responsiveness – while remaining physically present – produces immediate distress and physiological stress activation in infants within seconds [Grade A]. Clinical and field evidence suggests that a caregiver absorbed in a personal device replicates the Still Face condition in quotidian form: the body is present, but the face and relational availability are absent. Research on technoference confirms that parental mobile device use during caregiver–child interactions is associated with increased externalizing and internalizing behavioral problems in children as young as three years of age (McDaniel et al., 2026; McDaniel & Radesky, 2018) [Grade B–C].
Academic indicators tell a parallel story. In the United States, mathematics and reading scores measured by the National Assessment of Educational Progress reached their lowest levels in decades by 2022–2024 (NAEP, 2022, 2025) [Grade E]. Kuş (2025), a meta-analysis of 63 studies and 64 effect sizes including 124,166 students from 28 countries, found a small but statistically significant negative association between smartphone addiction, social media use, video-game use, and academic performance (Kuş, 2025; RADAM et al., 2026) [Grade B]. Sweden, having implemented one of the most ambitious digital-first education programs in the OECD, reversed this policy in 2026, mandating a return to paper, pens, and books and announcing a school smartphone ban effective August 2026 (Champion-Osselin, 2025).
1.2 A Rapidly Evolving Policy Landscape
The recognition that screen exposure constitutes a public-health concern is now reflected in legislation on a scale without historical parallel. UNESCO (2026) reports that as of March 2026, 114 education systems worldwide — representing approximately 58% of countries surveyed — have national mobile-phone restrictions or equivalent policies, up from approximately 60 at the end of 2023 and 79 at the end of 2024 (UNESCO, 2026). This near-doubling within two years marks the transition from scattered national experiments to an emerging global norm.
Policy movement has accelerated simultaneously across multiple regulatory domains. On school device restriction, major developments since the predecessor article include New Jersey joining the rapidly expanding U.S. state-level wave by requiring K–12 districts to adopt bell-to-bell restrictions on student use of cell phones and other internet-enabled devices for the 2026–2027 school year (NJDOE, 2026); Los Angeles Unified adopting district-wide classroom screen-time caps and restrictions on school-issued device use, the first major U.S. district to address school-issued screens alongside personal phones (Ede-Osifo, 2026); Brazil's Law No. 15,100 (in force January 2025), banning personal portable electronic devices in all public and private schools and requiring schools to develop mental health strategies and digital-addiction detection protocols (Pessoa, 2025); New Zealand's Education Review Office reporting 94% school adoption with 83% of secondary leaders noting improved focus and 69% reporting reduced bullying (ERO, 2025); Norway reaching 96% adoption in primary schools and 64% in secondary schools, with a quasi-experimental study finding causal effects of phone bans on reduced mental-health-care utilization in girls and improved GPA, particularly among low-SES students (Abrahamsson, 2024); and England's updated 2026 non-statutory guidance recommending full-day bans, alongside separate UK under-5 screen guidance issued in March 2026 capping exposure at one hour per day for ages 2–5 with explicit advice to avoid fast-paced social-media-style videos and AI toys/tools (Department of Education, 2026a, 2026b).
On age-based social media restriction, Australia introduced a platform-liability model — not a criminalization of child users, but a statutory obligation on age-restricted platforms to take reasonable steps to prevent under-16 account creation or retention, covering Facebook, Instagram, Snapchat, Threads, TikTok, Twitch, X, YouTube, Kick, and Reddit, with civil penalties of up to AUD 49.5 million per breach, in force from December 10, 2025 (eSafety Commissioner, 2026; UN, 2025). Within the first two months, Snapchat alone reported more than 415,000 locked accounts (AFP, 2026). Indonesia enacted equivalent restrictions for under-16s from March 28, 2026; Malaysia's Online Safety Act 2025 entered into force on January 1, 2026, with under-16 social media access restrictions being developed through subsidiary regulations (advancing/implementation pending) (MCMC, 2025); Denmark is advancing legislation for under-15s (Keaten, 2025); Turkey's parliament passed a bill restricting under-15 access in April 2026, pending final enactment (Wilks, 2026); and Austria has issued plans for an under-14 ban with draft legislation expected by end of June 2026 (AP News, 2026).
On early childhood institutional prohibition, France issued a ministerial decree prohibiting screen exposure for children under three years of age across all licensed early childhood settings – crèches, daycare centres, and registered childminders – including background sound, with very rare and adapted exceptions only for ages three to six, never during meals, before sleep, or for soothing (Ministère du Travail, de la Santé, des Solidarités et des Familles, 2025). This represents the flagship implementation of Model D (early childhood institutional prohibition) and the most direct regulatory translation of the zero-screen guidance for the most developmentally sensitive window. Madrid's regional government has established weekly screen caps in primary education, beginning with zero use for ages 0–3 and a maximum of one supervised hour per week for ages 3–6 (Jones, 2025).
On platform design regulation, the European Union's Digital Services Act (DSA) Articles 28 and 34 moved into active enforcement in 2025, requiring platforms to implement privacy-by-design defaults for minors, modify recommender systems, and conduct risk assessments for algorithmic content delivery to children (European Commission, 2025). Singapore introduced app-store-level Age Assurance Requirements via the IMDA Code of Practice for Online Safety for App Distribution Services (effective March 31, 2025), requiring system-level child-protection measures (IMDA, 2025).
A category of digital risk with no counterpart in the predecessor article has emerged as a significant concern: AI companion devices. Products marketed as screen-free and educational — voice-interactive plush toys, petbots, AI tutors – engage the child's attachment system through simulated emotional responsiveness and parasocial bonding dynamics, while delivering frictionless interactions that may displace the developmental friction through which empathy, conflict resolution, and pretend play are normally acquired (Common Sense Media, 2026; PIRG, 2025). AI companion devices represent an emerging high-concern category because they combine synthetic social contingency, personalization, and attachment-like engagement; the developmental risk is plausible and increasingly recognized in policy guidance (notably the UK 2026 under-5 guidance), but longitudinal evidence remains limited (Department of Education, 2026b).
1.3 The Conceptual Limitation of Existing Policy Frameworks
The acceleration of regulation has not been matched by a corresponding evolution in the conceptual models that inform it. The dominant policy metric remains a single quantity: hours of screen time per day or per week. This metric is administratively tractable and consistent across guidelines issued by the World Health Organization, the American Academy of Pediatrics, and national health authorities. It is also, the accumulated evidence indicates, insufficient as an index of developmental risk and may be actively misleading for the clinical subgroup discussed below.
We propose that the appropriate unit of analysis is not screen time but screen interaction: the total developmental exposure produced by a screen-mediated activity, defined by the intersection of multiple analytic dimensions rather than duration alone. Within this framework, the empirical case for distinguishing screen interaction from screen time is substantial. Sanders et al. (2019), drawing on data from 4,013 children, found that content type moderated developmental outcomes such that the aggregate hours variable predicted neither passive television's modestly negative effects nor educational screen use's small positive effects (Sanders et al., 2019) [Grade B]. Mallawaarachchi et al. (2024), in a meta-analysis of 100 studies and 176,742 participants, confirmed that content type, device type, and caregiver involvement each independently moderate outcomes, with identical aggregate duration producing developmentally divergent effects depending on context (Mallawaarachchi et al., 2024) [Grade B]. Lillard and Peterson (2011) demonstrated experimentally that nine minutes of fast-paced cartoon exposure produced significantly worse executive function performance in four-year-olds – a dose within every current guideline's permissible range (Lillard & Peterson, 2011)[Grade A].
Beyond this aggregation problem lies a more fundamental conceptual error: the treatment of screen exposure and screen addiction as differing only in quantity along a single continuum. Vezenkov and Manolova (2026), drawing on quantitative neurophysiological assessment of clinical cohorts of children with severe early screen addiction, propose that the prevailing discourse – framing the problem as "screen time" or "digital media use" – obscures an essential clinical reality: in a subgroup of children, a severe addiction has formed that systematically disrupts regulatory mechanisms and produces profound developmental disturbances (Vezenkov & Manolova, 2026) [Grade D]. Severe early screen addiction, in this clinical model, is defined not by hours of exposure but by compulsive seeking of high-intensity, low-social-density sensory stimulation; cycles of soothing followed by dysregulation; a shift of interest from human faces toward objects, colors, and repetitive sensory patterns; and a collapse of joint attention. Removing the device in these children produces withdrawal – not willful protest, but the loss of a regulatory prosthesis. This clinical model is supported by case-series and clinical-cohort evidence and remains to be prospectively validated in independent samples.
The framework explains why policies targeting only one dimension of screen interaction consistently produce smaller effects than anticipated. Goodyear et al. (2025), in the SMART Schools cross-sectional study of 30 schools and 1,227 students in England, found that restrictive school phone policies reduced in-school phone and social media use but were not associated with significantly better mental well-being, sleep, physical activity, or academic attainment (Goodyear et al., 2025) [Grade C]. Reynolds et al. (2025) reached a convergent conclusion from a meta-review and qualitative study in Ireland: students consistently identified workarounds, and total daily exposure was not meaningfully reduced (Reynolds et al., 2025). The implementation gap compounds the conceptual one: France's "Portable en pause" program was adopted by approximately 9% of collèges at the start of the 2025 academic year, with 67% of school directors stating they would not implement it (Morin, 2025) – illustrating the structural distance between legislative announcement and institutional adoption.
A further distinction structures the recommendations introduced in Section 8: the differentiation between euthymic screen time (EST) and hedonic screen time (HST), originally introduced by Manolova and Vezenkov (2025d) as a neurophysiologically grounded categorization. EST refers to screen engagement that is goal-directed toward a specific cognitive or communicative task with a defined endpoint, free from addictive design features (no autoplay, no infinite scroll, no variable reward, no algorithmic personalization), conducted in social context with an attentive adult, not deployed as a tool for emotional self-regulation, and — critically — characterized by preserved autonomic balance, sustained frontal cortical alertness, and the absence of significant dopaminergic perturbation. HST refers to screen engagement oriented toward pleasure, emotional relief, sensory stimulation, or psychophysiological state transition (tension to relaxation, boredom to excitement, wakefulness to sleep) – animations, gaming with variable reward, social media feeds, short-form algorithmically served video, pornography, gambling, AI companion devices – particularly when the content architecture is designed to sustain engagement beyond the user's conscious intention. HST disrupts autonomic balance through sympathetic or parasympathetic dominance, elicits significant dopaminergic engagement or a sedative profile depending on content, and, when sustained over months, produces what Manolova and Vezenkov term cortical sleep – a prolonged reduction of cognitive activation that constitutes the substrate of screen addiction. Importantly, EST is not a category that exists at every developmental stage: in children under approximately six years of age, cortical alertness and analytical capacity are insufficient for screen content to be processed non-hedonically, and all screen exposure in this age range functions as HST regardless of subject matter (Section 3.3). Recommendations that conflate these categories – as generic hourly limits invariably do – miss the mechanism that produces the greatest developmental harm (Manolova & Vezenkov, 2025d, 2025f; Petrov, Dimova, et al., 2025; Vezenkov & Manolova, 2026).
1.4 Aims of the Present Article
Three aims organize the present contribution.
First, we introduce a multidimensional screen interaction framework – defined by eight analytic dimensions, of which five have the strongest empirical support – and review the evidence base for each. This framework provides the interpretive lens for both the policy analysis and the clinical recommendations that follow.
Second, we examine the evidence on real-world implementation and effect of existing policies, drawing on published evaluations of school smartphone restrictions across multiple national contexts (Baggio et al., 2025; ERO, 2025; Goodyear et al., 2025; Reynolds et al., 2025), the initial compliance data from Australia's under-16 social media prohibition, and the literature on parental adherence to screen time guidelines.
Third, we introduce differentiated clinical recommendations for children in whom screen addiction or screen trauma has already formed – a population for whom generic time-limit guidance does not apply and for whom a specialized clinical pathway is required. This clinical contribution, derived from the work of the Vezenkov Center for Applied Neuroscience and grounded in the framework synthesized in Vezenkov and Manolova (2026) and the first volume of Nootism, represents the original scientific contribution of the present article to the international policy literature; we explicitly note its evidence base and validation status (Manolova & Vezenkov, 2025d, 2025e; Vezenkov & Manolova, 2025c, 2025b).
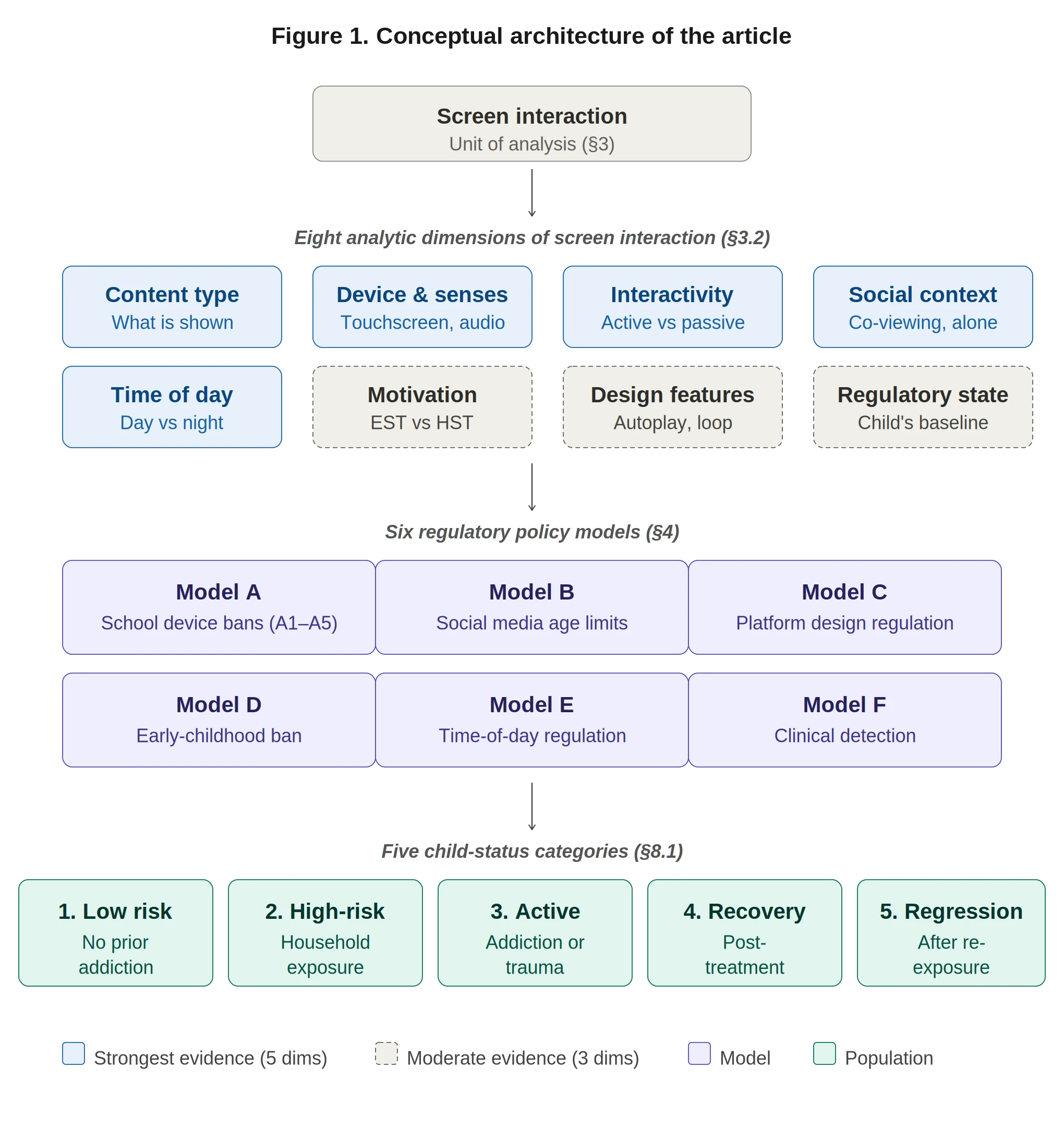
Figure 1. Conceptual architecture of the article. Screen interaction (Section 3) is decomposed into eight analytic dimensions (Section 3.2), of which five – content type, device and sensory affordances, interactivity, social context, and time of day – have the strongest empirical support, while three – motivational purpose (which operationalizes, together with design architecture and adult role, the EST/HST distinction of Section 3.3), design architecture, and the child's regulatory state – rest on more limited evidence. These dimensions inform six regulatory policy models (Section 4): school device restrictions (Model A, with subtypes A1–A5), social media age restrictions (Model B), platform design regulation (Model C), early-childhood institutional prohibition (Model D), time-of-day regulation (Model E), and clinical detection and health-system integration (Model F). Single-axis policies address only one or two dimensions each, which is the structural reason their aggregate effects on total daily exposure are smaller than anticipated (Section 5). Recommendations apply differentially across five child-status categories (Section 8.1), with categories 1–2 receiving regulatory and family-system interventions and categories 3–5 requiring clinical pathway management.
- Methods
2.1 Approach and Update Window
This article is a narrative review and policy mapping with a defined update window. Sources were searched, screened, and incorporated through May 10, 2026. The review combines five evidence streams: (i) peer-reviewed empirical research on the developmental effects of screen exposure; (ii) peer-reviewed and clinical-journal literature on screen addiction, screen trauma, and related clinical phenomena; (iii) intergovernmental and national policy documents (Department of Education, 2026a, 2026b; eSafety Commissioner, 2026; European Commission, 2025); (iv) primary legal sources (laws, decrees, ministerial guidance, government press releases); and (v) selected high-reliability media sources for very recent policy developments not yet captured in formal documentation.
Where multiple sources provided overlapping coverage of a single policy event, primary government or intergovernmental sources were preferred over media reports; peer-reviewed publications were preferred over preprints; and the most recent reliable source was used to establish current legal and implementation status. Where uncertainty about implementation status remained, this is noted explicitly in the text and in Appendix A.
2.2 Inclusion Criteria for Policy Measures
Policy measures were included if they met all of the following criteria: (a) target population includes children, adolescents, or settings where children are present; (b) regulatory mechanism addresses one or more of the following — school device access, social media age, platform design, early childhood institutional exposure, time-of-day access, or clinical detection and health-system integration; (c) legal or institutional status is documented through a primary government or intergovernmental source, or through a credible peer-reviewed or media account where primary documentation was not available; (d) the measure was enacted, published as binding guidance, or formally proposed within the period documented in the article (with proposal-status policies coded explicitly as such).
2.3 Policy Coding Framework
Each jurisdiction's measures were coded along the following parameters:
- Jurisdiction (national, sub-national, regional, supranational)
- Regulatory model (Model A: school device restriction, with subtypes A1–A5; Model B: social media age restriction; Model C: platform design regulation; Model D: early childhood institutional prohibition; Model E: time-of-day regulation; Model F: clinical detection and health-system integration)
- Legal status (in force / passed pending enactment / proposed / non-statutory guidance / advancing through subsidiary regulation)
- Effective date
- Age group / school level
- Scope (instructional time / bell-to-bell / breaks / extracurricular / off-school)
- Device or platform scope (personal smartphones / smartwatches / connected devices / school-issued devices / social media platforms / app stores)
- Enforcement mechanism (storage / collection / off-but-in-bag / platform liability / parental control / no specified mechanism)
- Exceptions (medical / disability / educational / emergency)
- Monitoring and evaluation (mandated longitudinal review / official press review / no formal monitoring)
- Evidence source (primary government document / intergovernmental source / peer-reviewed evaluation / media report)
The complete coding table is presented in Appendix A.
2.4 Evidence Grading
Each empirical claim in this article is graded by evidence type, applied to the original underlying study rather than to the article in which it is cited, using the following scheme:
|
Grade |
Evidence type |
|
Grade A |
Randomized controlled trial; quasi-experimental design with credible causal identification (instrumental variable, regression discontinuity, difference-in-differences); experimental laboratory study with random assignment |
|
Grade B |
Longitudinal cohort study; systematic review or meta-analysis of observational evidence |
|
Grade C |
Cross-sectional observational study; large representative survey |
|
Grade D |
Clinical cohort, case series, practice-derived biomarker evidence; specialized clinical population |
|
Grade E |
Government document, law text, intergovernmental report, media report, expert commentary |
This grading system enables readers to evaluate claims by the strength of their underlying evidence and prevents conflation of population-level associations with clinical-cohort observations. Notably, the Nootism clinical framework (Section 7) draws primarily on Grade D evidence – clinical cohort observations and biomarker case series – supplemented by convergent Grade A–C evidence from the broader neuroscience and developmental literatures. This grading is made explicit so that readers can distinguish the population-prevention recommendations (drawing on Grade A–C evidence) from the clinical-pathway recommendations (drawing on Grade D evidence with broader convergent support).
2.5 Operational Definitions
The article applies operational definitions throughout, summarized here for reference.
Screen interaction: the total developmental exposure produced by a screen-mediated activity, defined by the intersection of eight analytic dimensions (Section 3.2).
Euthymic screen time (EST): screen engagement that preserves autonomic stability and cortical alertness, with task-, learning-, or communication-oriented purpose, a defined endpoint, absence of addictive design features, active adult scaffolding, daytime timing, no role in emotional state regulation, and no significant dopaminergic perturbation. EST is not a category that exists below approximately six years of age (developmental threshold). Contraindicated at any dose in screen addiction or screen trauma. See operational table and developmental-threshold clause in Section 3.3.
Hedonic screen time (HST): screen engagement aimed at pleasure, soothing, reward, or psychophysiological state transition; characterized by open-ended use, presence of addictive design features (autoplay, feed, loot boxes, social metrics), absent or outsourced adult role, frequent evening or night timing, and use as a tool for emotional state regulation. Produces autonomic dominance (sympathetic or parasympathetic depending on individual and content), significant dopaminergic engagement or sedative effect, and, with sustained exposure, reduced cortical activation ("cortical sleep"). All screen exposure in children under approximately six years of age functions as HST regardless of content. Contraindicated at any dose in screen addiction or screen trauma. See Section 3.3.
Screen addiction: a clinical condition characterized by compulsive sensory seeking, withdrawal on device removal, collapse of joint attention, and measurable cortical and autonomic biomarkers, as defined in (Manolova & Vezenkov, 2025d, 2025f; Vezenkov & Manolova, 2025c, 2025b, 2026); not equivalent to heavy screen use.
Screen trauma: durable retuning of regulatory and sensory systems such that even after screens are removed, the person (child) remains anchored in infantile, sensory-dominant, dysregulated modes of functioning (Manolova & Vezenkov, 2025d; Vezenkov & Manolova, 2026).
Reversed development: a pathological reorganization in which evolutionarily older survival systems come to dominate higher human regulatory systems, with an inversion of the normative regulatory hierarchy (Manolova & Vezenkov, 2025f, 2025d; Vezenkov & Manolova, 2026).
2.6 Terminological Discipline for Causal Language
To prevent overstatement of causal claims relative to underlying evidence, the article applies a consistent terminological discipline:
- paralleled / coincided with — for historical co-occurrence of trends
- associated with — for cross-sectional or observational evidence
- predicted / preceded — for longitudinal evidence
- causally associated / estimated causal effect of — only for randomized, quasi-experimental, or natural-experiment evidence with credible causal identification
- clinical hypothesis / practice-derived model / case-series evidence — for the Nootism clinical framework, pending independent prospective validation
This terminological framework is applied throughout Sections 3–8 and is one of the safeguards against the conflation of population-level and clinical-cohort claims that the present revision aims to correct.
2.7 Limitations of the Method
The article is a narrative review rather than a systematic review, and it does not apply formal PRISMA procedures or pre-registered search strategies. The rapidly changing policy landscape – with new measures enacted within weeks of this article's update window – means some references reflect the best information available at the cut-off date and may have been superseded by subsequent developments. Several recent policies are documented through government press releases or media coverage rather than primary statutory text, particularly where laws have passed parliament but await final enactment. Self-reported screen-time data, on which much of the population-level evidence rests, systematically underestimate actual exposure (Júdice et al., 2023; Zhao et al., 2025). The clinical framework presented in Section 7 draws on specialized clinical cohorts at the Center for Applied Neuroscience Vezenkov and a developing clinical literature in Nootism; it requires independent prospective validation, and this limitation is noted explicitly throughout the relevant sections. A formal Limitations section (Section 9) returns to these issues at the conclusion of the article.
3. Conceptual Framework: From Screen Time to Screen Interaction
3.1 The Insufficiency of Duration as a Metric
The foundational premise of this section is that the quantity of time spent in front of a screen is not, on its own, a sufficient index of developmental risk or benefit. This position is not new: Sanders et al. (2019) demonstrated it empirically with data from 4,013 children in the Longitudinal Study of Australian Children [Grade B], and the research literature since has consistently reinforced it (Sanders et al., 2019). What is new is the urgency of drawing its policy implications, given that the global legislative wave documented in Section 1 is almost entirely organized around duration-based restrictions.
The core problem is that "screen time" aggregates exposure across categories whose developmental effects differ not merely in degree but in direction. Sanders et al. (2019) found that passive television viewing was associated with modestly negative outcomes on school-readiness measures, while educational screen use was associated with a small positive effect — and that the aggregate duration variable, averaged across both, predicted neither. Mallawaarachchi et al. (2024), in a meta-analysis of 100 studies and 176,742 participants, confirmed that content type, device type, and caregiver involvement each independently moderate outcomes, with identical aggregate duration producing developmentally divergent effects depending on context (Mallawaarachchi et al., 2024) [Grade B]. Lillard and Peterson (2011) demonstrated experimentally that nine minutes of fast-paced cartoon exposure produced significantly worse executive function performance in four-year-olds relative to educational programming or drawing — a dose well within every current guideline's permissible range (Lillard & Peterson, 2011) [Grade A].
A more fundamental conceptual error compounds the aggregation problem: the treatment of screen exposure and screen addiction as differing only quantitatively along a single continuum. Vezenkov and Manolova (2026), drawing on quantitative neurophysiological assessment of clinical cohorts, propose that this framing obscures an essential clinical reality: in a subgroup of children, a severe addiction has formed that systematically disrupts regulatory mechanisms and produces profound developmental disturbances (Manolova & Vezenkov, 2025b; Vezenkov & Manolova, 2025c, 2025e, 2025d, 2026) [Grade D]. The clinical model, its evidence base, and its limitations are addressed in detail in Section 7.
3.2 Screen Interaction: Eight Analytic Dimensions
We propose screen interaction as the appropriate unit of analysis, defined as the total developmental exposure produced by a screen-mediated activity. Screen interaction is characterized by eight analytic dimensions:
- Age of onset / developmental window – the developmental period during which exposure occurs, with strongest sensitivity in the first 1,000 days
- Motivational purpose – educational, communicative, soothing, or reward-seeking
- Content type – educational programming, entertainment animation, social media, gaming, short-form algorithmic video, AI companion content, pornography, gambling content
- Design architecture – autoplay, infinite scroll, variable reward schedules, recommender systems, social metrics, loot boxes, notification engineering
- Device and sensory affordances – television, tablet, smartphone, console, virtual reality headset, voice-interactive AI device
- Interactivity – passive reception, tool-like interactive use, algorithmically personalized engagement, synthetic-affective (AI companion) interaction
- Time of day and sleep proximity – daytime use, evening use, pre-sleep window, night-time use
- Social context and child neuroregulatory state – solo, caregiver co-present but inattentive, active co-engagement; and the child's pre-existing autonomic and regulatory profile, including whether screen-addiction functioning has already formed
The current evidence base is strongest for five of these dimensions – content type (3), device and sensory affordances (5), interactivity (6), social context (8 partial), and time of day (7) – which form the principal axes of differentiation in Section 6. Three dimensions – design architecture (4), motivational purpose (2), and the child's neuroregulatory state (8) – remain less systematically studied at the population level but are clinically and policy-relevant, and are addressed where evidence permits.
3.3 Euthymic Versus Hedonic Screen Time: Operational Definitions
Within the universe of screen interaction, the most clinically consequential distinction is between euthymic screen time (EST) and hedonic screen time (HST), originally introduced by Manolova and Vezenkov (2025d) as a neurophysiologically grounded — not merely behavioral — categorization of digital engagement (Manolova & Vezenkov, 2025d).
In the original formulation, EST denotes digital engagement that preserves autonomic stability and sustains cortical alertness: the frontal cortex remains engaged, autonomic balance is maintained, and dopaminergic regulation is not significantly perturbed. EST is therefore not associated with the emergence of screen addiction or its neurophysiological sequelae. HST denotes digital engagement aimed at inducing pleasure, relaxation, or — critically — a psychophysiological state transition (tension → relaxation, boredom → excitement, wakefulness → sleep). HST disrupts autonomic balance by producing dominance of either sympathetic or parasympathetic activity, elicits significant dopaminergic engagement with stimulating content or a sedative profile with passive content, and, when sustained over months, produces what Manolova and Vezenkov term cortical sleep — a prolonged reduction of cognitive activation that constitutes the cortical substrate of screen addiction.
A terminological clarification: "euthymic" as used here denotes screen engagement that is autonomically stable, cortically alert, non-compulsive, and developmentally proportionate; it does not correspond to the media-psychology meaning of "eudaimonic" (content oriented toward meaning and values). Some content that is thematically meaningful may be algorithmically delivered and architecturally designed to maximize engagement time, and therefore produces the autonomic and dopaminergic signature of HST regardless of subject matter.
To make this distinction operationally codable for family practice, clinical assessment, and policy design, we extend the original neurophysiological definition with the following measurable criteria (Table 1):
Table 1. Operational distinction between euthymic and hedonic screen time
|
Criterion |
EST |
HST |
|
Primary purpose |
Task, learning, communication, analysis |
Pleasure, escape, soothing, reward, state transition |
|
Endpoint |
Defined endpoint |
Open-ended |
|
Design features |
No autoplay, no infinite scroll, no variable reward, no algorithmic personalization |
Autoplay, feed, loot boxes, social metrics, algorithmic personalization |
|
Adult role |
Active adult co-engagement or scaffolding |
Adult absent, distracted, or outsourced to the device |
|
Time of day |
Daytime, outside transitions to or from sleep |
Frequently evening, night, or used as a transition into sleep |
|
Emotional function |
Not used to calm, feed, induce sleep, or manage distress |
Used to regulate distress, induce calm, or replace transition routines |
|
Autonomic signature |
Stable autonomic balance maintained |
Sympathetic or parasympathetic dominance; impaired state regulation |
|
Cortical signature |
Frontal alertness preserved; engagement of analytical networks |
Reduced cortical activation with sustained use (cortical sleep) |
|
Dopaminergic effect |
No significant perturbation of dopaminergic regulation |
Significant dopaminergic engagement or sedative effect, depending on content |
|
Clinical status |
Permissible only in absence of addiction or trauma, and only above the developmental threshold defined below |
Contraindicated in screen addiction or screen trauma at any dose |
Operational distinction between euthymic and hedonic screen time.
EST is defined by task-directed, bounded, adult-scaffolded engagement with preserved autonomic stability and cortical alertness. HST is defined by pleasure-, soothing-, reward-, or state-transition-oriented engagement, usually open-ended and architecturally reinforced by autoplay, feeds, variable reward, or algorithmic personalization. HST is contraindicated in screen addiction or screen trauma; EST is treated as developmentally unavailable below approximately six years within the framework proposed here.
Although the terms EST and HST retain the conventional phrase “screen time” for continuity with prior literature, they refer to categories of screen interaction rather than duration alone.
The developmental threshold. EST is not a category that exists at every developmental stage. The cortical alertness, analytical thinking, and interpretive capacity required to process screen content without entering hedonic state-modulation are not yet developed in children under six years of age; for this group, all screen exposure functions hedonically regardless of content (Manolova & Vezenkov, 2025d). The capacity for EST emerges gradually with cortical maturation and is the basis for the population-differentiated dosing introduced in Sections 8.2–8.3.
Time-to-addiction is asymmetric. Manolova and Vezenkov (2025d) note that the time required for HST to produce screen addiction varies systematically with age, autonomic and cortical maturity, gender, and lifestyle: the more developed and high-functioning the cortex, the slower addiction develops and the less severe its consequences. Younger and more rigid nervous systems develop addiction more rapidly and carry heavier sequelae, which is one of the principal reasons that under-6 exposure cannot be made safe through content selection alone.
This operationalization renders EST/HST a measurable framework rather than a terminological innovation, and it forms the basis for the population-differentiated recommendations in Section 8.
3.4 Why This Framework Matters for Policy
The eight-dimension screen interaction framework, with its EST/HST operationalization, has two specific implications for policy.
The first concerns displacement versus reduction. Policies that restrict access in one context – the school day, for example – without addressing content architecture, device affordances, or home social context do not reduce total developmental exposure; they redistribute it (Section 5). A policy that addresses only one or two dimensions of an eight-dimensional risk factor cannot be expected to produce aggregate effects proportionate to its political profile.
The second concerns the clinical exception. The framework above applies to children whose nervous systems have not been reorganized around screen-induced dysregulation. For children in whom early screen addiction or screen trauma has formed, the eighth dimension – pre-existing neuroregulatory state – becomes the primary determinant of any exposure's effect. For these children, even brief exposure to any form of screen content, including content that would qualify as EST for a neurotypical peer, can reactivate established compulsive and traumatic patterns (Petrova et al., 2025; Vezenkov & Manolova, 2025b, 2025e, 2026) [Grade D]. This population is the subject of Section 7 and of differentiated clinical recommendations in Section 8.
4. Global Policy Typology Updated to May 2026
4.1 Rationale
The international policy landscape is conventionally documented country-by-country, but country-level inventories conflate measures with categorically different regulatory mechanisms. A bell-to-bell physical confiscation policy is qualitatively distinct from a guidance document, even though both appear in counts of "countries with school phone bans"; an age-based statutory prohibition with platform liability operates through a different mechanism than a parental-consent-based access restriction; and a classroom-only restriction differs from a school-wide one in ways that materially affect downstream outcomes. This section therefore organizes the international landscape into six regulatory models, each defined by its primary regulatory mechanism. The complete coding table appears in Appendix A.
4.2 Model A: School Device Restrictions
Model A is the most widely adopted policy model globally. We distinguish five subtypes, each carrying different enforcement implications:
-
A1 – Classroom-only ban (devices prohibited during instructional time only; available during breaks/recess)
-
A2 – Bell-to-bell ban (devices prohibited throughout the school day, including breaks and extracurricular activities)
-
A3 – Storage-based policy (physical containment of devices at entry, regardless of A1/A2)
-
A4 – "Off but in bag" policy (devices may be brought but must remain powered off; the weakest variant)
-
A5 – School-issued device and classroom screen-time caps (limits on Chromebooks, tablets, and educational technology, distinct from personal-device restriction)
Subtype A5 is added in this version of the typology to capture an important regulatory innovation: many institutions ban personal phones while leaving school-issued tablets and Chromebooks as a continuous classroom screen presence. Los Angeles Unified became the first major U.S. district to address this dimension by adopting district-wide classroom screen-time limits, restricting elementary and middle-school device use during non-class time, and blocking YouTube on district devices (Ede-Osifo, 2026) [Grade E].
Europe
France introduced a classroom ban in nurseries, primary, and lower-secondary schools in 2018 (Law No. 2018-698), making it one of the earliest Model A adopters. The "Portable en pause" initiative, formalised through a circular of July 10, 2025, generalised the physical storage requirement — in locked pouches, lockers, or deposit boxes — to all collèges (lower secondary) from the start of the 2025–26 academic year. A pilot involving 200 collèges and 32,000 students in 2024–25 reported significantly improved school climate, reduced cyberbullying, improved concentration, and increased face-to-face interaction (Ministère de l'Éducation nationale, 2025) [Grade C]. However, a SNPDEN-UNSA survey in September 2025 found that only 8.5% of collèges had actually implemented the device at the start of the academic year, with 67% of head teachers stating they would not implement it — citing logistical complexity and absence of central funding — even though 42.8% supported the principle (SNPDEN-UNSA, 2025) [Grade C]. Additionally, from 20:00 to 07:00 and during weekends, the Ministry has introduced a default suspension of notifications on educational digital platforms (ENT/Pronote), constituting a novel Model E element targeting out-of-school digital disruption. A bill to extend the ban to lycées (upper secondary) was approved by the Assemblée nationale in January 2026 and by the Sénat on March 31, 2026, and is currently before a Commission Mixte Paritaire (CMP) with the aim of entry into force at the rentrée September 2026; teacher union SNPDEN-UNSA has raised concerns about enforceability and absence of resources (Franceinfo, 2026) (Morin, 2025) [Grade E]. Spain presents a sub-national convergence pattern analogous to Germany: there is no national school phone ban law, but the State School Council — the government's highest advisory body on education — unanimously recommended in January 2024 a total prohibition in preschools and primary schools and restrictions during school hours in secondary education (European Newsroom, 2024) [Grade E]. As of 2026, approximately 14 of Spain's 17 autonomous communities have implemented bans or restrictions, with full bans in preschool and primary being the predominant approach; notable early adopters include Castilla y León (2007), Castilla-La Mancha (2014), and Galicia (2015). The three remaining communities — Basque Country, La Rioja, and Navarre — have not enacted restrictions (UNESCO, 2025) [Grade E]. Implementation varies substantially: Murcia requires devices switched off in classrooms; Catalonia introduced a ban for primary schools from 2024–25; the Community of Madrid and Andalusia have regional regulations in place. Coded A1/A2 by region; no national law. Netherlands enacted A2 for secondary schools (January 2024) and primary schools (September 2024); approximately half of secondary schools have extended the ban to recess on their own initiative (Locker, 2024b). Belgium moved to a coordinated approach for 2025/26 across its three linguistic communities (Anas, 2025). Italy extended its primary/middle school ban to high schools in 2025 (Sevinc, 2025). Luxembourg introduced complete daytime ban under its Screen Life Balance campaign, effective April 2025 (RTL Today, 2025). Latvia enacted a ban for children up to Grade 6, effective October 2024 (Saeima Press Service, 2024). Portugal established a general rule prohibiting mobile phones in primary schools from 2025/26, with an evaluation of the preceding year's recommendations reporting 79% adoption for Years 1–4 and 41% for Years 5–6 alongside reductions in bullying and indiscipline (Eurydice Unit Portugal, 2025). Greece launched the "Cellphone in the School Bag" campaign in August 2024, following a joint announcement by Prime Minister Kyriakos Mitsotakis and Education Minister Kyriakos Pierrakakis. Students may bring phones to school but must keep them inside their school bags throughout the entire school day, including during lessons; there is no requirement to power devices off and no physical collection mechanism. The measure relies entirely on in-bag compliance, making it structurally equivalent to A4 — the weakest enforcement variant in the typology. Citing the scientific consensus on distraction and learning impairment, Mitsotakis stated that mobile phones "have no place in school during the school day." No penalty infrastructure or monitoring mechanism was announced alongside the campaign, placing implementation fidelity in question from the outset [Grade E]. Coded A1/A4. (Euronews, 2024). Hungary enacted legislation prohibiting smartphone use in schools, citing evidence of negative impacts on student attention and academic performance [Grade E]. The ban covers instructional time across all school levels; detailed enforcement provisions are not documented in available English-language sources. Coded A2 — enforcement fidelity unverified (Today, 2024). Austria issued a ministerial decree effective May 2025 for Grades 1–8 (O. M. | I. Wilkinson, 2025). Sweden announced a comprehensive bell-to-bell ban with mandatory physical collection effective autumn 2026 for ages 7–16 (Champion-Osselin, 2025). Finland enacted legislation in April 2025 with restrictions effective August 2025; uniquely, Finland's Department of Education and Culture has been tasked with carrying out a longitudinal impact study expected to report by end of 2026 (Bryant, 2025). Norway does not have a national law but has government-issued recommendations, with adoption reaching 96% in primary schools and 64% in secondary schools by 2024 (Locker, 2024c); the causal evidence is examined in Section 5. England updated its non-statutory guidance in 2026 recommending full-day bans (Department of Education, 2026a); separately, the UK government issued under-5 screen guidance in March 2026 (capping ages 2–5 at one hour daily, advising avoidance of fast-paced social-media-style videos and AI toys) – these two policies should not be conflated (Department of Education, 2026b). The United Kingdom presents a four-jurisdiction case study in the governance consequences of devolved education policy. England's Department for Education updated its non-statutory guidance in 2026, recommending full-day bans with physical enforcement; the guidance expects all schools to act in line with it, though legal compulsion remains absent (Department of Education, 2026a) [Grade E] — coded A2/A4 depending on school-level implementation. Scotland's national guidance (August 2024) explicitly stated that a national ban was "not appropriate or feasible," empowering headteachers and local councils to act independently (Scottish Government, 2024) [Grade E]; by early 2026, multiple councils had nonetheless introduced blanket bans, with the Yondr-pouch model being piloted in Edinburgh ahead of a projected city-wide rollout – a pattern of rapid sub-national convergence occurring in the absence of national mandate. A Scottish Parliament motion in October 2025 calling for a statutory classroom ban was defeated, with the government citing teacher professional autonomy (Scottish Parliament, 2025) [Grade E]. Wales had, as of March 2026, no national ban, with individual schools retaining decision-making authority; a dedicated stakeholder forum had produced a first draft of national guidance (Welsh Government, 2026) [Grade E]. Northern Ireland published guidance in September 2024 recommending that pupils avoid phone use during the school day, without mandating enforcement mechanisms (Department of Education Northern Ireland, 2024) [Grade E]. The UK's four-nation divergence illustrates a recurring structural feature of federal and devolved systems: the absence of a national mandate does not prevent sub-national convergence, but it produces uneven adoption rates and a "postcode lottery" of school environments – a pattern also documented in Germany, Australia, and the United States. Denmark reached a legislative political agreement in autumn 2025 to make all primary and lower secondary schools mobile-free from the 2026–27 academic year; students will be required to hand in phones and tablets at the start of the school day. The agreement is grounded in data showing that over 50% of students in grades 6 and 8 reported being distracted by screens during lessons. Simultaneously, Denmark announced an investment of 540 million DKK over ten years to replace classroom tablets and laptops with physical textbooks — one of the most substantial national reversals of a digital-first education policy documented in any European country [Grade E]. The Well-Being Commission additionally recommended that children under 13 should not own smartphones. Coded A2 — pending formal legislative enactment. (Barrett, 2025). Poland has fast-tracked a school smartphone ban for September 2026 [Grade E]. Coded A2 — pending implementation. (Reuters, 2026). Russia enacted a lesson-time ban in 2023, covering instructional time in all state schools [Grade E]. Coded A1 (Locker, 2024a). Ireland does not have a statutory national school phone ban as of May 2026. Reynolds et al. (2025) — one of the key Model A implementation studies reviewed in Section 5 — documents sub-national Irish school policies operating on a school-discretion basis, with findings indicating that students find workarounds and that restrictions produce small or no effect on total daily use [Grade C]. Ireland therefore presents a case analogous to Norway: widespread informal practice in the absence of a national legislative mandate. Coded sub-national A1/A2 (school-discretion).
Germany has no federal school device policy; constitutional competence for education rests entirely with the sixteen Länder, producing a patchwork of state-level measures. Hesse is among the more advanced Länder adopters, implementing school device restrictions with reported positive feedback from school administrators [Grade E]; coding varies by municipality. Bavaria issued school phone guidelines as early as 2006; several other Länder have issued guidance without statutory basis. The absence of a national German policy is analytically notable given Germany's size and the EU-wide trend: it illustrates how constitutional structure shapes the political feasibility of model adoption independently of evidence or political will. Coded A1–A2 (Länder-dependent); no national coding applicable (Pugh, 2026).
Asia-Pacific
Singapore tightened guidelines from January 2026 for secondary school students, prohibiting smartphone and smartwatch use during the entire school day — including recess, co-curricular activities, and supplementary lessons – with devices stored in lockers or school bags; schools may grant exceptions where necessary [Grade E]. Primary school restrictions (lesson-time only) have been in place since January 2025. Singapore's IMDA Code of Practice for Online Safety for App Distribution Services entered force on March 31, 2025, addressing app-store-level child protection (IMDA, 2025) [Grade E]. Additionally, the default Device Management Application sleep hours on government-issued Personal Learning Devices were moved from 23:00 to 22:30 from January 2026, representing a rare instance of Model E time-of-day regulation applied through centrally managed educational device infrastructure rather than through commercial platform obligations (MOE, 2025) [Grade E]. These three measures are coded distinctly: A1 (primary), A2 (secondary), C (IMDA), and E (DMA sleep hours). South Korea enacted a revision to the Elementary and Secondary Education Act in August 2025, banning mobile phones and smart devices during class hours in all elementary, middle and high schools, effective March 1, 2026 — the day before the new school year [Grade E]. The law passed with bipartisan support (115–31, with 17 abstentions). Exceptions are permitted for students with disabilities, educational purposes, and emergencies. Teachers are granted authority to restrict devices; schools are tasked with promoting responsible digital habits. The legislation formalises informal restrictions already in place at many schools, providing uniform legal basis nationwide. South Korea presents a uniquely acute context for this policy: 99% of South Koreans are online and 98% own a smartphone, the highest rate among 27 countries surveyed by Pew Research (2022–2023); Ministry of Education data indicate that 37% of middle- and high-school students report social media affecting their daily lives and 22% report anxiety when unable to access social media [Grade C]. Youth advocacy groups have challenged the law as a violation of children's human rights (Ji-hye, 2025) [Grade E]. The 2026 school ban represents South Korea's second major regulatory intervention in digital access by minors — following the Shutdown Law (Model E, 2011–2021) — and marks a shift from time-of-day gaming regulation to classroom device restriction. Coded A1, not A2. China, while limited at the national level, saw Zhengzhou become the first Chinese city to legislate a school phone ban in primary and secondary schools in 2025 (Chen, 2025). Japan – the Prefecture of Kagawa enacted a formal ordinance in 2020 establishing parental responsibility for limiting screen and gaming time for residents under 20, capped at 60 minutes on weekdays and 90 minutes at weekends. The ordinance also introduced a device curfew: children under 15 were prohibited from device use after 21:00, and those aged 15–18 after 22:00. Notably, the ordinance contains no enforcement mechanism — compliance is delegated entirely to parents — a structural feature that places it in the category of legislative declaration rather than implemented regulation. The ordinance was passed despite a 600-signature public petition calling for its withdrawal (Hoppe, 2020) [Grade E]. Saudi Arabia implemented a ban in 2021 (Hilotin, 2025). United Arab Emirates — The UAE Ministry of Education has prohibited the bringing of mobile phones onto school premises entirely, with accompanying regulations establishing procedures for inspection and confiscation of devices found in students' possession. School administrators retain the authority to designate exceptions in cases of documented educational necessity (Hilotin, 2025) [Grade E]. Coded A2/A3. Pakistan (Punjab Province) — The Punjab Higher Education Department issued a resolution banning mobile phones in all public and private schools and colleges in Pakistan's most populous province, citing the disruptive effect of social media use during lectures and the impact of teacher device use on classroom atmosphere. The measure extends the prohibition to both students and teaching staff — one of the few jurisdictions globally to include educators explicitly in the scope of a school device ban, alongside Bangladesh (Hilotin, 2025) [Grade E]. Coded A2. India – the state of Andhra Pradesh enacted a ban on mobile phone use by both students and teachers in schools in 2023. In March 2025, the Delhi High Court declined to impose a total smartphone ban nationwide, instead issuing a set of guidelines governing permissible school smartphone use — the first documented instance of a national court explicitly rejecting a total prohibition in favour of a graduated regulatory framework (Hilotin, 2025) [Grade E]. The Delhi ruling is analytically significant: alongside the Kagawa constitutional litigation (Section 5.2), it constitutes one of only two recorded cases of a formal legal challenge to the principle of school device restriction, and the only case in which a court substituted a regulatory framework for the total ban sought by the applicants. Coded A1 (Andhra Pradesh); judicial guidance framework (Delhi). Bangladesh introduced its first classroom ban on mobile phone use by both teachers and students in 2011, via a Ministry of Education circular — one of the earliest such measures globally. This was extended in 2017 to a comprehensive prohibition on bringing phones into schools and colleges entirely (bdnews24.com, 2011; BBC News, 2023) [Grade E]. Bangladesh thus predates France (2018) as a national-level school device restrictor, though enforcement consistency across its extensive public school system has not been systematically evaluated. Coded A2.
The Americas
Brazil enacted Law No. 15,100 (in force January 2025) prohibiting portable electronic devices in public and private elementary, middle, and high schools during classes, recess, and breaks — with exceptions for pedagogical use, emergencies, accessibility, and health needs. The law is notable for combining the device ban with statutory requirements for schools to develop mental health strategies, train staff to detect signs of psychological distress, and create dedicated student support spaces, positioning it between Model A and Model F (Library of Congress, 2025) [Grade E]. Implementation began in February 2025; approximately two-thirds of Brazilian schools had already applied some form of restriction prior to the law, providing a higher baseline of compliance than most comparable national rollouts (Euronews, 2025) [Grade E]. A September 2025 survey by the Parliamentary Front for Education (n = national sample) found that 80% of students reported improved classroom concentration, with 77% of school administrators and 65% of teachers reporting reductions in cyberbullying; 44% of students reported increased boredom during breaks — a finding consistent with the displacement pattern identified in Section 5 (Albuquerque, 2025) [Grade C]. A differences-in-differences study of Rio de Janeiro's earlier phased school phone ban — classroom-only from August 2023, extended school-wide from February 2024, which preceded and directly inspired the 2025 national law — finds that test scores in math and Portuguese improved by 0.06 standard deviations in schools without prior strict phone rules relative to schools that already had them; extrapolating to a full-compliance counterfactual suggests total gains on the order of 0.2 standard deviations, comparable in magnitude to the effect of reducing class size in Project STAR. The study covers grades 6–9 across 325 municipal schools and 196,757 students, representing the largest municipal school district in Latin America (Lichand et al., 2026) [Grade A]. Coded A2 + F. United States – with no federal legislation, the USA presents the most extensive sub-national policy landscape globally. As of February 17, 2026, 41 states have enacted laws or policies governing student cellphone use in K-12 public schools (Ballotpedia, 2026) [Grade E]. Of these, 32 states ban or actively restrict cellphone use, 5 states require districts to adopt their own policies without specifying their content, and 4 states issue encouragement or guidance only. Florida's HB 379 (May 2023) was the first state law enacted nationally, passed unanimously by both chambers [Grade E]. The pace of adoption accelerated dramatically in 2025, with the majority of currently active laws enacted within a single legislative year. Key state-level developments include: New York's bell-to-bell restrictions for the 2025–26 school year, with approximately USD 13 million allocated statewide for storage infrastructure and a separate SAFE for Kids Act restricting algorithmically curated feeds for under-18s without parental consent; California's Phone-Free School Act requiring all districts to adopt restriction policies by July 2026; New Jersey's ban signed January 2026 (S3695); Michigan's classroom ban signed February 2026 (HB 4141, effective 2026–27); and North Dakota, which uniquely mandates that districts collect and report data on the effects of the ban on student mental health, attendance, and academic performance – the only state-level evaluation mandate in the country. Physical enforcement infrastructure is supported by dedicated public funding in several states: Pennsylvania allocated USD 100 million for a school phone-pouch grant program, and Delaware and Arkansas have established similar pilot schemes [Grade E]. Los Angeles Unified became the first major U.S. district to address school-issued device screen time, adopting district-wide classroom screen-time limits and blocking YouTube on district devices – coded as Model A5 (Ballotpedia, 2026) [Grade E]. Canada – with education a provincial jurisdiction and no federal legislation, Canada presents a sub-national policy landscape comparable in structure to the United Kingdom and the United States. Ontario was the first Canadian province to restrict phone use in schools (2019); its policy was strengthened in September 2024 to a full-day ban for grades K–6 and a classroom-only ban for grades 7–12, with social media blocked on all school networks [Grade E]. British Columbia implemented a bell-to-bell ban across all school districts from fall 2024. Alberta introduced an instructional-time ban for K–12 with network-level social media blocking from fall 2024. Saskatchewan and Nova Scotia apply classroom bans for all grade levels. New Brunswick requires devices to be silenced and stored during class. Quebec enacted a classroom ban from January 2024, escalating to a full bell-to-bell ban covering all school grounds – including hallways, the schoolyard, and breaks – from September 18, 2025 (Éducaloi, 2025) [Grade E]. One-year implementation data from Quebec indicate faster-than-anticipated student compliance when bans are province-mandated rather than school-managed, alongside reported increases in extracurricular participation and face-to-face socialization; violations are sanctioned with suspension (Sharma, 2026) [Grade C]. Four Ontario school boards, including the country's largest (Toronto District School Board), filed lawsuits against Facebook, Instagram, Snapchat and TikTok in March 2024, the first such litigation in Canada, alleging harm to student mental health [Grade E]. As of May 2026, Ontario is considering extension to a near-total ban on all school property; Manitoba is advancing plans to ban social media and AI chatbots in classrooms. The four territories (Yukon, NWT, Newfoundland and Labrador, Nunavut) have not yet legislated in this area [Grade E]. Coded A1–A2 varying by province. Chile enacted legislation in December 2025 prohibiting smartphone and connected device use during curricular activities across all school levels – preschool, primary, and secondary – effective from the 2026 school year, pending promulgation by President Boric; schools have until mid-2026 to update internal compliance policies [Grade E]. The law was adopted with overwhelming cross-party support following years of lobbying by parents and teachers; more than half of Chilean students reported device-related disruption to learning in the most recent OECD/PISA data. A Santiago school had previously piloted cellphone signal-blocking – an enforcement mechanism distinct from the physical-storage approaches dominant in Europe – prior to national legislation [Grade E]. Coded A1. Argentina — with education a provincial jurisdiction, Argentina presents a sub-national policy pattern analogous to Canada and the United States. Two distinct measures are in force. The Autonomous City of Buenos Aires issued a ministerial resolution in August 2024 restricting phone use in all schools across kindergarten, primary, and secondary levels: in kindergartens and primary schools, phone use is strictly prohibited during classes and breaks; at secondary level, devices must be stored during lessons unless explicitly authorized for educational activities; each institution defines its own enforcement procedures and consequences; students with disabilities requiring devices are exempt [Grade E]. Separately, the Province of Buenos Aires has adopted a ban on mobile phones in primary schools (UNESCO, 2026) [Grade E]. No national legislation exists; the two Buenos Aires jurisdictions should not be conflated, as they cover different populations and school levels. Coded A1/A2 (city) and A2 (province, primary only).
New Entrants (UNESCO, 2026)
UNESCO additionally records new national bans in Bolivia, Costa Rica, Croatia, Georgia, Maldives, and Malta, with school-level mandates in Colombia, Estonia, Lithuania, Iceland, Peru, Indonesia, Serbia, Poland, and the Philippines. Documentation for these jurisdictions in English-language primary sources is limited; most are captured through UNESCO's quarterly tracking database and government press releases rather than statutory text or peer-reviewed implementation studies. Where mechanism information is available from the database: Croatia, Estonia, and Lithuania each report classroom-level bans (A1) with no specified storage infrastructure; Malta and Georgia report school-wide restrictions (A2); Colombia and Peru report guidance-level measures without statutory basis (equivalent to A4 in enforcement terms). The cluster of adoption across Latin America (Bolivia, Colombia, Chile, Peru, Argentina), the Pacific (Philippines, Maldives), and South-East Europe (Croatia, Serbia, Georgia) reflects a second wave of Model A diffusion, predominantly following the 2023 UNESCO global recommendations and the 2024–25 high-profile enactments in France, Australia, and Brazil. The absence of implementation evidence for this cluster means their inclusion in counts of "countries with school bans" substantially overstates the documented regulatory floor; pending independent evaluation, they are classified Grade E throughout.
4.3 Model B: Social Media Age Restrictions
Model B prohibits or restricts the creation and maintenance of social media accounts by minors below a defined age threshold. Four distinct enforcement mechanisms can be identified across current implementations: (i) platform liability — statutory obligations on platforms to prevent minor account creation, with civil penalties for non-compliance (Australia, UK); (ii) risk-based access differentiation — tiered access levels by platform risk profile rather than binary prohibition (Indonesia); (iii) age-gating with eKYC — government-identity-linked verification as the operative mechanism (Malaysia, Turkey); and (iv) parental consent — requiring explicit guardian authorisation for account creation, without a hard prohibition (France, Singapore, Canada). These mechanisms are not mutually exclusive; several jurisdictions combine elements. A cross-cutting distinction is whether enforcement burden rests on platforms, on parents, or on users — with platform liability models representing the highest-accountability variant and parental-consent models the lowest, given the structural asymmetry between platform resources and individual family capacity to enforce compliance.
Australia introduced the world's first platform-liability model — not a criminalization of child users, but a statutory obligation on age-restricted platforms to take reasonable steps to prevent under-16 account creation or retention. Coverage includes Facebook, Instagram, Snapchat, Threads, TikTok, Twitch, X, YouTube, Kick, and Reddit; civil penalties reach AUD 49.5 million per breach; in force from December 10, 2025 (eSafety Commissioner, 2026) [Grade E]. The eSafety Commissioner's three-month review identified persistent "poor practices" by some platforms; Snapchat reported 415,000+ locked accounts in the first two months (AFP, 2026).
Indonesia enacted Government Regulation No. 17 of 2025 (PP Tunas — Tata Kelola untuk Anak Aman dan Sehat Digital), signed by President Prabowo Subianto on March 28, 2025 as a derivative of Indonesia's Personal Data Protection Law; enforcement commenced March 28, 2026 following a one-year transition, operationalised through Ministerial Regulation No. 9 of 2026 (Groen, 2026) [Grade E]. Indonesia is the first country in Southeast Asia and the first non-Western country to implement age-based social media restrictions at national scale. Unlike Australia's threshold-based model, Indonesia applies a risk-based framework: children aged 13–16 face differentiated access levels by platform risk profile. Eight platforms were designated high-risk and required to deactivate accounts of under-16 users: YouTube, TikTok, Facebook, Instagram, Threads, X, Bigo Live, and Roblox [Grade E]. At the enforcement date, X and Bigo Live were assessed as compliant; Roblox and TikTok as partially compliant, with remediation plans submitted (Groen, 2026) [Grade E]. Indonesia has approximately 299 million internet users; official data indicate approximately 50% of surveyed Indonesian children had been exposed to sexual content online (Cosseboom, 2026) [Grade C]. The Ministry conducted a surprise inspection of Meta's Jakarta office ahead of the announcement, signalling an assertive enforcement posture. Amnesty International and digital-rights organizations have raised concerns that the measure constitutes a "quick fix" that does not address the structural platform-design conditions producing harm (Groen, 2026) [Grade E]. Coded B. Malaysia's Online Safety Act 2025 received Royal Assent in May 2025 and entered into force on January 1, 2026, placing proactive obligations on platforms to prevent under-16 account access. The operative under-16 restriction is being introduced through subsidiary legislation — a Child Protection Code and Risk Mitigation Code — with implementation expected by mid-2026 following an MCMC public consultation period of 12 February to 31 March 2026 (FMT, 2026; Mayer Brown, 2025) [Grade E].
The Malaysian model is framed as "delay, not ban" — restricting independent account management rather than imposing a total prohibition — with eKYC using government-issued identification (MyKad, passport, MyDigital ID) as the primary age-verification mechanism [Grade E]. The UN Committee on the Rights of the Child (February 2026) expressed concern about inadequate digital inclusion safeguards and recommended a child-rights-based approach; Amnesty International Malaysia and civil society coalitions have raised constitutional concerns about the use of subsidiary legislation to introduce restrictions that may contradict the parent Act, and questioned proportionality (Edward, 2026) [Grade E]. Coded B — advancing/implementation pending as of May 2026.
Singapore introduced Age Assurance Requirements via the IMDA app-store code (March 2025), reflecting an "L-plate" graduated model rather than a binary ban (IMDA, 2025; TechPolicy.Press, 2026).
United Kingdom — the Online Safety Act 2023, Phase 1, placed Ofcom-enforced duties on platforms to protect children from illegal and harmful content, with Children's Safety Codes requiring age assurance, safer algorithms, and default privacy settings for under-18 accounts; Ofcom enforcement of the children's duties began in 2024 [Grade E]. Phase 2, anticipated late 2026, is expected to introduce criminal liability for senior platform managers for serious harm to children (noted under Model C). The OSA's child-protection obligations constitute a hybrid B/C measure: platform liability for minor access to harmful content (B), combined with design-architecture requirements (C). Coded B/C.
France has required parental consent for users under 15 to register on social media since 2023 (Geographical, 2023). The same parliamentary bill advancing in 2026 also proposes prohibiting social media platform services for users under 15 from September 1, 2026, enforced by ARCOM; the Sénat version introduces a distinction between "blacklisted" harmful platforms and others requiring parental consent, creating a difference with the Assembly version that the CMP must resolve (Localtis, 2026) [Grade E].
Spain is advancing legislation to raise the minimum social media age from 14 to 16, requiring explicit parental consent and effective platform age verification (La Moncloa, 2025) [Grade E]. Coded B — advancing.
Brazil enacted Law No. 15.211/2025, the Digital Child and Adolescent Statute (ECA Digital), on 17 September 2025. The law establishes a broad framework for protecting children and adolescents in digital environments, including platform obligations concerning protective design, parental tools, transparency, advertising/monetisation, and loot boxes. This measure is distinct from Law No. 15.100/2025, the school-device restriction law; it should therefore be coded B/C rather than conflated with school-device regulation.
Denmark's government announced a political agreement on November 7, 2025, to ban social media for users under 15, backed by a parliamentary majority spanning multiple parties. A limited parental opt-in is available for ages 13–14 following a specific assessment. The minister cited data indicating 94% of Danish children under 13 already have at least one social media profile as justification for the measure. Formal legislation was in parliamentary process as of May 2026; the digital affairs minister signalled months would be needed to close loopholes for tech platforms (Keaten & Press, 2025) [Grade E]. Coded B — advancing/legislative process.
Turkey's Grand National Assembly adopted legislation on April 23, 2026, prohibiting social media platforms from providing services to users under 15, requiring platforms to implement age verification systems, and mandating differentiated services with mandatory parental controls — including usage time monitoring, account management, and consent for purchases — for users aged 15–17 (AP News, 2026a; Balkan Insight, 2026) [Grade E]. The law entered a 15-day presidential approval period; if signed, it enters into force six months after publication in the Official Gazette, projecting to approximately October 2026. All users — not just minors — must verify their identity through Turkey's e-Devlet government portal, which generates a unique key while preventing platforms from accessing underlying personal data; no comparable democracy has yet paired child-protection legislation with universal identity verification of this kind (The Next Web, 2026) [Grade E]. Companies with more than 10 million daily users must comply with content removal orders within one hour; foreign services with more than 100,000 daily users must maintain a local representative; gaming platforms must age-classify all games. Enforcement is through Turkey's communications regulator BTK, with penalties escalating from advertising bans to bandwidth throttling to access bans — the same graduated mechanism previously used against platforms that declined to comply with political content removal orders (The Next Web, 2026) [Grade C]. The immediate political trigger was the Kahramanmaraş school shooting of April 14, 2026, in which a 14-year-old killed nine students and a teacher. The main opposition CHP has stated that children should be protected "with rights, not bans" (Al Jazeera, 2026) [Grade E]. Coded B; in force approximately October 2026.
Austria has issued plans for an under-14 social media ban, with draft legislation expected by end of June 2026 – this is not yet law (AP News, 2026b) [Grade E]. Coded B – draft only.
United States – no national restriction. State-level measures include New York's SAFE for Kids Act (algorithmic feed restrictions for under-18s without parental consent) and California's Age-Appropriate Design Code (Governor Hochul, 2025); constitutional constraints make federal legislation unlikely (Kang, 2024). Coded B/C (state-level, varying).
A cross-cutting implementation challenge is age-verification effectiveness; current verification systems (self-declaration, credit-card linkage, government ID upload, biometric estimation) each carry significant limitations and are circumvented by VPN use (EFF, 2025). The EU's planned Age Verification Application (late 2026 pilot) and Digital Identity Wallets, Turkey's e-Devlet integration, and Malaysia's MyKad eKYC system represent the most technically developed responses, each reflecting different trade-offs between verification robustness, privacy protection, and civil liberties.
4.4 Model C: Platform Design Regulation
Model C represents the most technically sophisticated regulatory approach and, in the view of several policy analysts, the one most closely targeted at the actual mechanism of harm – the addictive design features embedded in platform architecture (Vezenkov & Manolova, 2026). Rather than restricting access by age or location, Model C requires platforms to modify the design of their products: disabling autoplay, infinite scroll, variable-reward notification schedules, and algorithmically personalized feeds for minor users. From the screen interaction framework advanced in Section 3, this is the most consequential regulatory direction, because design architecture is the dimension on which population-level policy can most directly act to reduce the share of screen engagement that meets the operational criteria for HST in Section 3.3 – and, in particular, to prevent the algorithmic and variable-reward features that drive the autonomic, cortical, and dopaminergic signature of HST at scale. The section below notes cross-references where jurisdictions coded primarily under Model B (UK OSA Phase 1, New York SAFE for Kids Act, Singapore IMDA, Brazil Law 14,811) also carry Model C obligations; those entries are detailed under Section 4.3.
European Union — DSA Articles 28 and 34, in active enforcement from 2025, require Very Large Online Platforms to implement privacy-by-design defaults for minors, modify recommender systems, and conduct risk assessments for algorithmic delivery to children (Digital Strategy, 2025). The European Commission published implementation guidelines in 2025, and enforcement proceedings against several platforms were initiated in 2025. A pilot EU Age Verification Application is announced for late 2026, involving France, Spain, Italy, Greece, and Denmark; EU Digital Identity Wallets are expected from end of 2026.
China's minor mode represents the most developed Model C technical system globally. Initially proposed as draft guidelines in August 2023, CAC published final guidelines in November 2024 and launched minor mode on April 29, 2025 — a mandatory device-level framework requiring smartphones to include a configurable minor mode with age-specific content restrictions (under-3s: music/audio only; ages 12–16: educational/news content), daily time caps (under-8: 40 min; ages 8–15: 1 hour; ages 16–17: 2 hours), a 22:00–06:00 service blackout with exemptions for educational tools and emergencies, break reminders every 30 minutes, and parental override options (ITIF, 2025; CAC, 2024) [Grade E]. The 2021 gaming restriction, in force since August 2021, limits minors under 18 to three hours of online gaming weekly — playable only from 20:00 to 21:00 on Fridays, Saturdays, Sundays, and public holidays — enforced through mandatory real-name registration (NPPA, 2021) [Grade E]. China's Regulations on the Protection of Minors Online entered force in January 2024, with implementing draft measures for platform identification published September 2025 (CAC, 2025) [Grade E]. All three instruments operate within a state-surveillance context that other jurisdictions do not replicate and that raises distinct human rights concerns absent from other Model C implementations.
Spain's draft digital protection law includes two Model C provisions: (i) a requirement that all digital devices sold in Spain include free, accessible parental control systems pre-configured during initial device setup — a device-level implementation of minor-mode principles; and (ii) a prohibition on minors accessing video game loot boxes — randomized in-game purchases whose variable-reward mechanics are structurally equivalent to gambling and produce the same dopaminergic sensitisation (La Moncloa, 2025; Vezenkov & Manolova, 2026) [Grade E]. The loot box prohibition is the most direct legislative application of behavioral-addiction science to platform design available in any current jurisdiction. Coded C (advancing).
New York's SAFE for Kids Act prohibits social media platforms from serving algorithmically curated addictive feeds to users under 18 without explicit parental consent, targeting the recommendation architecture directly rather than access (Governor Hochul, 2025) [Grade E]. This measure is cross-coded B/C: listed under Model B (Section 4.3) but the operative obligation is a design-architecture requirement — the clearest example in the US context of Model C regulation. Coded C (in force).
California's Age-Appropriate Design Code (AB 2273) requires platforms likely to be accessed by minors to implement privacy-protective defaults, disable features that profile or nudge children, conduct Data Protection Impact Assessments prior to launching products or services likely to be accessed by minors, and provide clear information about data practices in age-appropriate language (Governor of California, 2022) [Grade E]. The law is subject to ongoing constitutional litigation; enforcement was stayed pending judicial review in 2023, with reinstatement proceedings underway as of 2025. Coded C (litigation-constrained).
United Kingdom's Online Safety Act Phase 2, anticipated late 2026, is expected to introduce criminal liability for senior platform managers in cases of serious harm to children — shifting enforcement liability to individuals rather than organizations, a structural escalation beyond civil financial penalties [Grade E]. OSA Phase 1 children's safety duties and Ofcom's Children's Safety Codes (cross-coded B/C, detailed in Section 4.3) are already in force from 2024. Coded C (Phase 1 in force; Phase 2 advancing).
The expected EU Digital Fairness Act (Q4 2026) is anticipated to address deep fakes, child-directed influencer marketing, and dark-pattern design.
4.5 Model D: Early Childhood Institutional Prohibition
Model D policies specifically target screen exposure during the earliest developmental window — the period Vezenkov and Manolova (2026) identify as carrying the greatest risk of severe and least reversible developmental harm, because the nervous system's foundational regulatory, attentional, and social architectures are being laid down and are maximally sensitive to environmental disruption. This model remains the least developed globally: most jurisdictions that have enacted Model A or B measures have not extended their regulatory reach to the 0–6 age group in institutional settings, and the WHO recommendations that would most directly motivate such measures have not been updated since 2019 despite substantial evidence development. The entries below record the important recent precedents.
France stands as the flagship Model D implementer. A ministerial decree, framed explicitly within France's national policy for the first 1,000 days of life, prohibits any screen exposure for children under three years of age across all licensed early childhood settings — crèches, daycare centres, and registered childminders — including background television and audio, in force from July 3, 2025 (Ministère du Travail, 2025) [Grade E]. For ages 3–6, exposure is permitted only very rarely, with an adult present and using adapted content; explicitly prohibited during meals, before sleep, and as a soothing or transitional tool (Ministère du Travail et des Solidarités, 2025) [Grade E]. Coded D (in force).
Spain (Madrid region) has established weekly screen caps across primary education anchored at zero for ages 0–3, rising to a maximum of one supervised hour per week for ages 3–6, and up to 90 minutes per week for school Years 3–4, with a prohibition on screen-based homework across all primary levels (The Guardian, 2025) [Grade E]. The weekly-measurement approach — rather than a daily cap — limits cumulative exposure while permitting concentrated educational use when genuinely needed. Coded D (regional regulation).
Bulgaria has had a Health Ministry regulation since 2023 establishing tiered educational screen use limits in nurseries and kindergartens: up to 10 minutes once weekly for ages 2–3; twice weekly for ages 3–5; and twice weekly for ages 5–7 — all strictly for educational purposes and to be followed by at least 90 minutes of physical activity [Grade D]. Bulgaria is notable as the only jurisdiction outside France with a national-level quantified limit on institutional screen exposure for under-3s, and the specific sequencing requirement (physical activity following screen use) reflects a clinically grounded approach to autonomic recovery. Coded E (in force) (Petrov, Dimova, et al., 2025).
Taiwan was the first country globally to treat excessive child screen time as a legally regulated harm: a 2015 legislative amendment classified excessive screen time as comparable to other addictive behaviors, exposing parents to fines for screen-related harm to children (Chibber & Quartz, 2015) [Grade E]. The measure targets parental behavior rather than licensed settings and is therefore a hybrid D/E measure rather than a pure institutional prohibition. Coded D/E (in force since 2015).
England — the UK Department for Education issued under-5 screen guidance in March 2026, the most detailed national guidance for this age group produced by any Anglophone government (Department of Education, 2026b) [Grade E]. The guidance caps screen time for ages 2–5 at one hour daily, advises complete avoidance for under-2s, specifically warns against fast-paced social-media-style videos and AI companion toys, and recommends no screen use in the two hours before sleep and no screens in children's bedrooms. Non-statutory, but should not be conflated with the separate Model A school device guidance also issued in 2026 (Department of Education, 2026a). Coded D (non-statutory guidance).
Sweden's public health agency (Folkhälsomyndigheten) issued guidelines recommending zero screen time for under-2s and a maximum of one hour daily for ages 2–5, explicitly addressing parental screen use in the child's presence as a developmental risk factor distinct from the child's own use (The Guardian, 2024) [Grade E]. Coded D (guidance).
Norway's government-appointed Screen Use Committee (2024) recommended severely limiting screen time for children under two years of age, applying a precautionary-principle framework given the absence of evidence for developmental benefit in this age group (Norwell, 2024) [Grade E]. Coded D (recommendation).
WHO guidelines (2019) recommend no sedentary screen time for under-2s and a maximum of one hour per day for ages 3–4, with a strong preference for interactive activities with a caregiver over passive viewing (WHO, 2019) [Grade E]. These recommendations are the most widely cited normative reference point for Model D policy-making globally, yet have not been updated since 2019 despite substantial evidence development — including the neuroimaging studies reviewed in Sections 6.2–6.3 and the clinical evidence in Section 7. The absence of an updated WHO guideline is itself a governance gap, leaving national regulators without a contemporary authoritative benchmark.
4.6 Model E: Time-of-Day Regulation
Model E policies restrict screen access during specific hours of the day, most commonly the night-time period. As established in Section 6.5, time of day is an independent axis of developmental risk, operating through melatonin suppression, cortisol elevation, and displacement of pre-sleep co-regulation behaviors that are critical for both sleep architecture and learning consolidation (Beyens & Nathanson, 2019; Vezenkov & Manolova, 2026). The Japanese polysomnographic evidence (PMC 7916284, 2021) indicates that time of use – specifically within two hours of sleep – is a stronger predictor of sleep quality than total daily screen duration, making Model E a potentially high-leverage intervention even without overall duration limits. Despite this evidence base, formal Model E legislation outside China remains sparse: home-based night-time screen use is one of the most developmentally consequential dimensions of screen interaction yet one of the least accessible to regulatory intervention without either platform-enforced curfews or parental control mandates.
China is the most comprehensive Model E implementer globally through two distinct mechanisms. The minor mode's mandatory 22:00–06:00 service blackout, applicable to all smartphones in minor mode, entered force on April 29, 2025 (ITIF, 2025; CAC, 2024) [Grade E]. Separately, the 2021 gaming restriction — limiting minors to three hours of online gaming weekly, playable only from 20:00 to 21:00 on permitted days — includes an implicit nighttime prohibition as a structural consequence of the weekly time cap (NPPA, 2021) [Grade E]. Both instruments operate within a state-surveillance context absent from other Model E implementations. Coded E (in force; cross-coded C).
South Korea's "Shutdown Law" / "Cinderella Law" (2011–2021) is the earliest and most extensively documented example of Model E regulation globally. The Youth Protection Revision Act of 2011 prohibited online PC gaming for users under 16 between midnight and 06:00, enforced through South Korea's mandatory 13-digit resident registration number system. Violations by game companies carried fines of up to ₩10 million (~$8,560 USD) or up to two years imprisonment; both PSN and Xbox Live enforced the curfew for underage Korean accounts. The law emerged following multiple deaths linked to MMO addiction. However, its effectiveness waned as mobile games — exempt from the law — grew to represent 54% of the gaming market by 2018, and minors shifted to social media and video streaming. Children also bypassed the system via parental ID numbers or foreign servers. The law was repealed in 2021 and replaced by an opt-in "Choice System" allowing parents or legal guardians to designate permitted gaming hours. South Korea remains a key case study illustrating both the rationale and the practical limits of time-of-day digital regulation (Sang et al., 2016; BBC, 2021; Korea Herald, 2021).
Japan (Toyoake City, Aichi Prefecture) – in October 2025, Toyoake City enacted an ordinance establishing a recommended two-hour daily limit on recreational smartphone use for all residents, with particular application to children and teenagers. The ordinance introduces a time-of-day dimension: elementary school students are advised to avoid smartphone use after 21:00, and junior high school students and older after 22:00. The measure carries no penalties and relies on family-level compliance — a structural feature shared with the 2020 Kagawa ordinance. Toyoake represents a second sub-national Japanese Model E initiative, notable for its extension beyond gaming to recreational screen use broadly defined and for its explicit targeting of evening and night-time use as the primary risk window (Gulf News, 2025) [Grade E].
Singapore — the default sleep hours on the Device Management Application installed on all government-issued Personal Learning Devices were moved from 23:00 to 22:30 from January 2026 — a rare instance of Model E time-of-day regulation applied through centrally managed educational device infrastructure rather than through commercial platform or parental control obligations (MOE, 2025) [Grade E]. Cross-coded A (Section 4.2). Coded E (in force).
England's 2026 under-5 screen guidance explicitly recommends no screen use in the two hours before sleep and that screens be excluded from children's bedrooms at night — the most specific pre-sleep window recommendation issued by any Anglophone national government (Department of Education, 2026b) [Grade E]. Non-statutory; cross-coded D. Coded E (guidance).
Sweden's public health agency (Folkhälsomyndigheten) guidelines recommend no screen use before bedtime and no screens in children's bedrooms across all age groups (The Guardian, 2024) [Grade E]. Cross-coded D. Coded E (guidance).
The governance gap that characterizes Model E — substantial developmental evidence, sparse binding legislation — reflects a structural feature of the regulatory terrain: night-time home screen use is the dimension most proximate to the mechanism of harm yet most insulated from state intervention by household privacy norms. The two pathways available for closing this gap — platform-enforced curfews embedded in device-level minor modes (the Chinese model) and parental control mandates with default-on settings (the direction of Spain's draft law and Singapore's DMA) — each involve trade-offs between effectiveness and civil liberties that no jurisdiction outside China has yet fully resolved.
4.7 Model F: Clinical Detection and Health-System Integration
Model F is the least developed globally and the one most directly connected to the clinical framework advanced in this article. It refers to the integration of screen addiction and screen-induced developmental harm into formal health-system pathways: screening, assessment, referral, and treatment. The distinction between Model F and the other five models is that Models A–E seek to prevent or restrict screen exposure in specific contexts, while Model F responds to the developmental harm that has already occurred – identifying affected children, connecting them to clinical services, and building the professional and institutional infrastructure to deliver effective intervention. The near-absence of Model F infrastructure globally is the most consequential gap in the current regulatory landscape, because the population of children for whom prevention-oriented measures are insufficient – those with established screen addiction or screen trauma – has no systematic clinical pathway in any jurisdiction outside the documented examples below.
Spain is the most advanced Model F implementer. The draft digital protection law explicitly requires pediatricians and other health professionals to incorporate questions about screen and internet usage into routine examinations, enabling early identification and intervention for digital addiction, with referral pathways to clinical support (La Moncloa, 2025) [Grade E]. The law additionally prohibits minors from accessing video game loot boxes, on the grounds that their variable-reward mechanics are structurally equivalent to gambling — an explicit acknowledgement in statute that platform design features constitute an addiction risk requiring clinical management, not only consumer protection. Coded F (advancing; cross-coded C for the loot box provision).
Brazil's Law No. 15,100 (in force January 2025) includes school-level clinical detection mandates: schools are required to train staff to detect signs of psychological distress related to digital overuse and to create dedicated student support spaces for those affected (Library of Congress, 2025) [Grade E]. This partial Model F integration within a Model A framework is analytically significant — it is the only national school ban law globally that explicitly combines access restriction with a detection and support obligation, positioning the school as the first point of contact in a clinical pathway rather than merely a restriction context. Coded F (in force; cross-coded A).
South Korea has operated the most institutionally developed non-clinical Model F system globally since the early 2010s. Following the introduction of the Shutdown Law (Model E, 2011), the government established a national internet and gaming addiction screening infrastructure: the National Information Society Agency (NIA) developed and validated the Korean Internet Addiction Scale (K-Scale) and its derivatives for different age groups; mandatory screening was introduced in school health checks; and a network of counselling and treatment centers — the Internet Addiction Prevention and Counselling Centers — was established under Ministry of Science and ICT oversight. The Korea Mental Health Crisis Counselling Centre has run a dedicated digital addiction helpline since 2012. South Korea thus represents the only jurisdiction globally with a population-level screening tool, a mandated school-health integration point, and a publicly funded specialist referral network operating simultaneously as a Model F system [Grade E]. The repeal of the Shutdown Law in 2021 did not dismantle this infrastructure; the voluntary Choice System that replaced it explicitly relies on the counselling network to support families (Korea Herald, 2021). Coded F (in force).
The Vezenkov Center for Applied Neuroscience in Sofia, Bulgaria, operates the most comprehensive documented clinical pathway for screen addiction and screen trauma assessment and treatment currently available in the peer-reviewed literature. The pathway includes qEEG and HRV-based biomarker assessment; the SIPVR and SIPECR screening instruments; total digital detox protocols; and the Nootism therapeutic framework for full regulatory recovery (Vezenkov & Manolova, 2026) [Grade D]. The clinical recommendations developed in Sections 7 and 8 of this article are derived from this pathway. Independent prospective validation across multiple sites is the stated research priority. Coded F (operational; provides the clinical evidence base for Sections 7–8).
The governance gap that defines Model F is structural rather than informational: the evidence that a subpopulation of children requires clinical intervention rather than behavioral guidelines has been available for over a decade, yet no national health system outside South Korea has embedded screen addiction screening into routine pediatric care, and no jurisdiction outside Spain has legislated a referral pathway. The implication — developed fully in Section 8 — is that the current global policy wave, concentrated in Models A and B, is addressing the accessible regulatory surface while leaving untouched the population for whom these measures are both insufficient and potentially contraindicated: children whose nervous systems have already been reorganised around screen-induced dysregulation.
4.8 Supranational Frameworks
Several supranational regulatory frameworks deserve separate treatment, as they operate above the national level and set the normative context — and in some cases the legal obligation — within which national policies are adopted. Their significance varies: some are binding on member states (EU DSA), some establish normative standards that inform domestic legislation without legal compulsion (UN Committee on the Rights of the Child, Council of Europe), and some provide tracking and advocacy functions without regulatory authority (UNESCO, UNICEF).
UNESCO issued a global recommendation for mobile phone bans in schools in 2023 and has tracked adoption quarterly since, reporting 114 educational systems with national bans or equivalent measures as of March 2026 — up from 60 at the end of 2023, representing a near-doubling in under three years (UNESCO, 2026) [Grade E]. UNESCO frames the issue primarily in terms of educational quality and child well-being, without addressing the clinical distinction between screen use and screen addiction; its tracking database consequently conflates measures with categorically different regulatory mechanisms — the typological problem this article addresses in Section 4.1. UNESCO's role as a normative agenda-setter is significant: the 2023 recommendation provided political cover for a second wave of national adoptions, particularly across Latin America, South-East Europe, and the Pacific.
World Health Organization guidelines (2019) recommend no sedentary screen time for under-2s and a maximum of one hour per day for 3–4-year-olds, specifying that where screen time does occur for older toddlers it should be interactive and co-viewed with a caregiver rather than passive solo viewing (WHO, 2019) [Grade E]. These recommendations have not been updated since 2019 despite substantial development in the evidence base — including the neuroimaging studies reviewed in Section 6 and the clinical biomarker evidence in Section 7. The absence of a WHO update is a governance gap with direct consequences: national regulators rely on the WHO standard as the primary international benchmark for Model D policy-making, yet the 2019 document predates the systematic evidence on short-form algorithmic video, AI companion devices, and the neurophysiological biomarkers of early screen addiction.
European Union — the DSA framework (detailed in Section 4.4) represents the most legally developed supranational regulatory instrument for platform-level child protection. Its combination of risk assessment obligations (Article 34), design requirements (Article 28), and enforcement capacity — significant fines and injunctions against VLOPs, with penalties calculated as a percentage of global annual turnover — positions it as the most consequential ongoing regulatory development in the field globally (Digital Strategy, 2025) [Grade E]. Enforcement proceedings against TikTok and Meta platforms were initiated in 2025. The expected EU Digital Fairness Act (Q4 2026) will extend the framework to deepfakes, child-directed influencer marketing, and dark-pattern design.
UN Committee on the Rights of the Child — General Comment No. 25 (2021) on children's rights in relation to the digital environment is the most comprehensive supranational normative statement on the subject available [Grade E]. It establishes that states have obligations under the Convention on the Rights of the Child to protect children from harm in digital environments; regulate the design and operation of digital products and services; ensure algorithmic systems serve children's best interests; require data minimisation and privacy-by-default for minor users; and provide effective remedies for digital rights violations. General Comment No. 25 provides the human rights law foundation for Models B, C, and F, and has been cited in domestic legislation and court proceedings across multiple jurisdictions. It explicitly addresses the tension between child protection and children's right to participate in digital life — the same tension raised by youth advocacy groups challenging bans in South Korea and Japan (Section 4.2).
UNICEF issued a warning in December 2025 that age-related social media bans will not keep children safe, cautioning that blunt access restrictions without addressing platform design, digital literacy, and underlying mental health factors risk pushing children toward unmoderated spaces while failing to address the structural conditions of harm (UN, 2025) [Grade E]. UNICEF's position is the most prominent institutional counterweight to the Model B adoption wave and directly echoes the displacement concern raised by the Australian implementation evidence in Section 5.6. It does not argue that Model B measures lack merit; it argues they are insufficient in isolation — a conclusion convergent with the multi-axis intervention framework advanced in Section 8.
Council of Europe — Recommendation CM/Rec(2018)7 on Guidelines to respect, protect and fulfil the rights of the child in the digital environment provides a pre-legislative normative framework that anticipated many of the design-architecture obligations now being enacted through the DSA and national Model C measures. The Lanzarote Committee (monitoring body for the Convention on Protection of Children against Sexual Exploitation and Sexual Abuse) has increasingly addressed online grooming and digital access as implementation issues intersecting with Model B age-restriction debates. The Budapest Convention on Cybercrime (in force in 68 states as of 2025) establishes the criminal law framework within which digital child protection enforcement operates. These instruments collectively constitute the international legal architecture within which national Models A–F are situated, and explain why the displacement of enforcement burden from states to platforms — the direction of Models B and C — has proceeded faster in Council of Europe member states than in most other regions.
5. Implementation Evidence
5.1 The Policy–Implementation Gap
Documenting enacted legislation is not equivalent to documenting change. The policy landscape mapped in Section 4 represents, to a significant degree, a record of political intention rather than measured developmental impact. The two are related but not equivalent: a law that is unenforced, circumvented, or unevenly adopted produces different effects from a law that is implemented with fidelity; and even a well-implemented law may produce different effects from those its framers intended if it addresses only one dimension of a multidimensional risk factor.
This section assembles the available evidence on what actually happens after screen policies are introduced: how consistently they are adopted by the institutions they target; how reliably they reduce exposure in the contexts they govern; whether that contextual reduction translates into a corresponding reduction in total daily exposure; and what the downstream effects on well-being, mental health, and academic outcomes have been where these have been measured. The evidence base is uneven — school device restriction policies have been studied more extensively than any other model — and the methods range from quasi-experimental natural experiments to cross-sectional surveys and qualitative accounts. Claims are reported with the evidence qualifications their design warrants.
The central empirical pattern is precise: policies are necessary but not sufficient. School device restrictions reliably reduce device access in the governed context, but their effects on total daily exposure, well-being, academic outcomes, sleep, and bullying depend on enforcement fidelity, policy design, implementation duration, school culture, and home-environment displacement. The framework is not "works/doesn't work"; it is "works under what conditions, for which outcomes, on what time horizon." More fundamentally: policies address the context of exposure without consistently addressing its total volume, and they address the accessibility of devices without addressing the content architecture that drives compulsive use. The conceptual framework developed in Section 3 — particularly the distinction between displacement and reduction, and the recognition that screen addiction requires a clinical pathway rather than a regulatory intervention — provides the explanatory basis for both what the evidence shows and what it implies for policy design.
5.2. Legal and Civil Resistance as an Implementation Constraint
A dimension of the policy–implementation gap that is systematically underreported is resistance from those the policies target. The Kagawa case is the most documented example. Following adoption of the 2020 ordinance, a 17-year-old resident identified publicly only as Wataru initiated crowd funded constitutional litigation challenging the ordinance on the grounds that it infringed the constitutionally guaranteed right to self-determination. His attorney argued that rules governing device use should be determined by individual families rather than by government mandate. Wataru also contested the scientific basis of the measure, stating that the correlation between gaming time and adverse outcomes does not constitute evidence of causation, and noting that for some young people, gaming functions as the primary available coping mechanism for pre-existing stressors such as school-related difficulties (Hoppe, 2020).
The Kagawa litigation is significant for three reasons. First, it is the earliest documented case of a minor mounting a formal legal challenge to a screen time regulation, establishing a precedent for rights-based contestation of this category of law. Second, the absence of an enforcement mechanism in the ordinance itself – explicitly acknowledged by the prefecture – reflects a pre-emptive accommodation of the legitimacy concerns that the litigation later articulated. Third, the argument that screen use may function as adaptive coping for a subpopulation of at-risk adolescents – rather than as the source of harm – anticipates the clinical framework developed in Section 7 of the present article: screen addiction and screen trauma are not products of duration alone, but of the interaction between content architecture, developmental vulnerability, and the social-emotional conditions of the user's environment.
5.3 Parental and Family Adherence to Screen Time Guidelines
A meta-analysis in JAMA Pediatrics drawing on 95 samples and 89,163 children found that only 24.7% of children under two years met the zero-screen recommendation, and only 35.6% of children aged two to five met the one-hour daily limit (McArthur et al., 2022) [Grade B]. The French ELFE birth-cohort study (n>18,000) found only 13.5% adherence to the no-screen recommendation for children under two (Lapierre et al., 2022) [Grade B]. A global review of adherence to combined 24-hour movement guidelines for ages 5–17 found an overall adherence rate of approximately 7.6% (Frontiers in Public Health, 2024) [Grade B].
Low adherence reflects structural rather than informational factors. Hamilton et al. (2015) found that parental awareness of recommendations had only a modest association with child screen exposure [Grade C]. Brown and Smolenaers (2016) identified a specific cognitive distortion among parents: many did not count their own device use in the child's presence as "screen time" — though developmentally, parental device use during caregiver–child interaction constitutes technoference regardless of intent. Self-reported screen time substantially underestimates objective exposure (Radesky et al., 2020; Zhao et al., 2025) [Grade C]. The single strongest population-level predictor of child screen exposure is parental screen use (Lapierre et al., 2022; Wen et al., 2025).
5.4 School Device Restrictions: Evidence by Strength of Design
The available studies on school device restrictions vary substantially in design and consequently in causal warrant. Table 2 organizes the principal evidence.
Table 2. School device restrictions
|
Study / Context |
Design |
Main result |
Use |
|
Goodyear et al. (2025) – SMART Schools, England |
Multi-method cross-sectional observational study (n=1,227, 30 schools) |
Less in-school phone and social media use; no significant difference in mental well-being, sleep, physical activity, academic attainment |
Establishes that school ban alone, in absence of platform/home intervention, does not produce well-being or attainment effects [Grade C] |
|
SSRN (2025) – Norway |
Quasi-experimental / event-study using variation in ban timing |
Reduced healthcare take-up for psychological symptoms in girls; reduced bullying; improved GPA and academic-track probability; effects larger for low-SES girls |
Strongest available positive causal evidence [Grade A] |
|
NBER (2025) — Florida |
Quasi-experimental |
Short-term suspensions increase, then decline; test scores improve in year 2; unexcused absences decline |
Indicates transition costs and delayed benefit [Grade A] |
|
SIEPR (2025) — Stanford / Yondr pouches |
Quasi-experimental, large administrative data |
Reduced phone use; no immediate broad academic effect; student well-being higher by year 3; disciplinary problems initially up then down |
Indicates enforcement works, outcomes lag [Grade A] |
|
Baggio et al. (2025) — South Australia |
Emulated trial (n=1,062), pre–post comparison |
Reductions in psychological distress |
Suggestive positive effect; vulnerable to secular trend confounding [Grade B–C] |
|
Reynolds et al. (2025) — Ireland |
Meta-review and qualitative study |
Students find workarounds; small/no effect on total daily use |
Convergent with SMART Schools displacement finding [Grade C–D] |
|
Beland & Murphy (2016) — London |
Quasi-experimental |
Improved attainment, largest effects for lowest-achieving students |
Earlier positive evidence; pre-smartphone-saturation context [Grade A] |
|
Bhargava et al. (2022) — Catalonia/Galicia |
Pre–post comparison |
Improved grades; reduced cyberbullying |
Suggestive positive evidence [Grade C] |
|
Kemp et al. (2024) — PISA cross-country |
Cross-sectional, with controls |
Schools with bans show lower results when gender, SES, prior behavior controlled |
Suggests selection effects in non-experimental studies [Grade C] |
|
ERO New Zealand (2025) |
Government implementation review |
94% schools enforce full-day bans; 83% leaders report improved focus; 69% report reduced bullying; ~50% of secondary students consistently follow rules |
High adoption-fidelity reporting; mixed compliance [Grade E] |
|
Government of South Australia (2025) |
Government 12-month review |
93% leaders report incident decline; 34% reduction in violations |
Implementation positive; outcome data limited [Grade E] |
|
Edweek Research Center (2026) — U.S. |
Survey of teachers and leaders |
64% teachers report consistent enforcement; 36% report inconsistent |
Documents enforcement asymmetry [Grade E] |
|
Le Monde (2025) — France |
Government announcement; press tracking |
9% of collèges adopted; 67% of directors stated they would not |
Documents the policy–implementation gap [Grade E] |
The single most important methodological correction relative to the predecessor article concerns the SMART Schools study: it is a multi-method cross-sectional observational study, not a randomized controlled trial, and should be cited as such (The Lancet Regional Health – Europe, 2025).
5.5 What the Evidence Shows About Mechanisms
Three mechanisms recur across the available evidence and require explicit articulation.
Displacement, not reduction. The SMART Schools and Reynolds findings indicate that school restrictions reduce in-school phone use without reducing total daily phone or social media use; students compensate before school, on the journey home, and in the evening (Goodyear et al., 2025; Reynolds et al., 2025; Goodyear et al., 2026). From the screen interaction perspective, this is the expected outcome of a policy addressing only the context dimension while leaving content, design, interactivity, and home social context unchanged.
Enforcement architecture determines fidelity. Bell-to-bell storage-based policies (A2+A3) reliably reduce in-school use; "off but in bag" policies (A4) are effectively unenforceable (Marshall, 2026; Edweek Research Center, 2026; Government of South Australia, 2025). This pattern justifies a more precise policy formulation: the effective unit is not "ban / no ban" but "ban + storage + enforcement + adult modelling + parent communication + monitoring."
Outcome benefits lag implementation. The SIEPR and NBER evidence indicates that disciplinary, attainment, and well-being effects emerge gradually — sometimes only by the second or third year of policy implementation, and sometimes preceded by a transition period of increased disciplinary action. This lag has implications for political evaluation: policies should not be judged on first-year outcomes alone.
5.6 Social Media Age Restrictions: Early Implementation Evidence
Australia's three-month implementation review (eSafety Commissioner, 2026) identified persistent "poor practices" by some platforms and no measurable reduction in cyberbullying complaints in the initial period. Snapchat reported 415,000+ locked accounts in the first two months (Financial Times, 2026); platform compliance — account removal — is not equivalent to safety, since excluded minors may migrate to unmoderated alternatives. This displacement risk is analogous to the content-displacement problem in school device restriction.
Age-verification circumvention is a structural feature, not a contingent failure, of current Model B implementations. VPN downloads among Australian adolescents increased markedly following implementation (EFF, 2025). The EU's planned Age Verification Application and Digital Identity Wallets represent the most promising technical direction.
5.7 Platform Design Regulation: Emerging Evidence
Model C policies have the least implementation evidence but address the mechanism of harm most directly. China's gaming restrictions and minor mode have produced reductions in officially measured metrics, partially offset by VPN-based migration and substitution to non-restricted forms of HST. The EU DSA has generated initial enforcement proceedings, but systemic effects on platform design will take several years to characterize. New York's SAFE for Kids Act, in initial implementation, is the most precisely targeted measure available; outcome evidence is not yet available.
5.8 Five Conclusions from the Implementation Evidence (Table 3)
-
School device restrictions reliably reduce in-school use under storage-based enforcement, but do not reliably reduce total daily exposure. The strongest exception is Norway (causal positive evidence, particularly for low-SES girls).
-
Social media age restrictions face structural circumvention challenges in the near term, particularly in absence of interoperable verification infrastructure.
-
Parental adherence to screen guidelines is consistently low across all studied national contexts, reflecting structural rather than informational factors.
-
Single-axis policies produce displacement; total-exposure effects require multi-axis intervention.
-
No existing regulatory measure adequately addresses the needs of children with established screen addiction or screen trauma, who require a clinical pathway rather than a behavioral guideline.
Table 3
|
Policy focuses |
What it captures |
What it misses |
|
Daily screen-time limit |
Duration |
Content, timing, design architecture, addiction status |
|
School phone ban |
School context |
Home displacement, school-issued device exposure |
|
Social media age ban |
Account access |
Gaming, video, AI companions, circumvention |
|
Parental control software |
Household device access |
Parental modelling, caregiver technoference |
|
Platform safety regulation |
Content harms |
Autonomic regulation, early childhood exposure |
|
Clinical treatment |
Affected child |
Public prevention infrastructure |
6. Differential Developmental Effects of Screen Interaction
6.1 Rationale and Scope
Section 3 introduced the eight-dimension screen interaction framework. The present section reviews the empirical literature underlying the five dimensions with the strongest evidence base — content type, device and sensory affordances, interactivity, social context, and time of day — and notes the more limited evidence on the remaining three dimensions where relevant. The aim is to enable the reader to locate the specific evidence behind each claim, with explicit grading.
A preliminary methodological observation: research in this field carries systematic limitations. Self-reported screen time substantially underestimates objective exposure (Radesky et al., 2020; Zhao et al., 2025) [Grade C]; most studies are cross-sectional; "screen time" is operationalized inconsistently; and the fastest-changing exposure categories (algorithmically served short-form video, AI companion devices) are the least studied because the research cycle lags platform innovation. These limitations are noted where relevant; stronger causal claims are reserved for Grade A studies with experimental or quasi-experimental design.
6.2 Content Type
6.2.1 Educational Versus Passive Entertainment
Sanders et al. (2019) [Grade B] demonstrated that content type moderates outcomes in ways that aggregate duration concealed: passive television was associated with modestly negative effects on school readiness; educational screen use was associated with a small positive effect; aggregate hours predicted neither. Madigan et al. (2019) [Grade B] found that screen time at 24 and 36 months was associated with lower performance on developmental screening at 36 and 60 months across language, motor, social, and problem-solving domains. Mallawaarachchi et al. (2024) [Grade B], in the most comprehensive meta-analysis available (100 studies, 176,742 participants), found that program viewing, background TV, age-inappropriate content, and caregiver screen use during child interactions were each independently associated with worse cognitive and psychosocial outcomes; co-viewing with active engagement was associated with better cognitive outcomes – identical aggregate hours, structurally divergent effects.
6.2.2 Fast-Paced Content and Acute Executive Function Effects
Lillard and Peterson (2011) [Grade A] randomly assigned four-year-olds to nine minutes of fast-paced fantasy cartoon, educational cartoon, or drawing, and found significantly worse executive function in the fast-paced cartoon group. The dose was nine minutes – within every current guideline's permissible range – making this finding directly policy-relevant: content architecture and pace can produce acute neurocognitive effects independent of any cumulative-exposure mechanism.
6.2.3 Early Video Exposure and ASD-Like Symptom Profiles
Heffler [Grade B], in prospective studies, found that television and video exposure at 12 months predicted ASD-like symptoms at 24 months in a dose-dependent manner (Heffler et al., 2020, 2022, 2024). The authors hypothesized that early audiovisual exposure redirects the developing social attention system away from face-and-voice processing and toward object-and-motion processing – the social orientation profile characteristic of ASD. Law et al. (2023) [Grade C] found that infant screen use was associated with altered EEG markers (increased theta power, altered functional connectivity) at 18 months and with lower performance on cognitive outcomes – providing direct neurophysiological evidence in humans that early screen exposure is associated with measurable cortical organization differences (Law et al., 2023a).
These findings converge with the clinical framework of Vezenkov and Manolova (2026) [Grade D], who propose that early screen exposure reorients the mirror neuron system (System 0) away from human microsignal processing – faces, gaze, pause, rhythm – toward 2D, accelerated, edited input. In their account, the screen does not prevent imitation; it changes its target. When this retuning is severe and early, it produces the social orientation profile that clinically maps onto ASD presentations across all three DSM-5 clusters: failures of social reciprocity (System 0 distortion), repetitive and ritualistic behavior (System 1 dominance), and a picture not fully explained by global developmental delay (System 2 stall). Manolova and Vezenkov [Grade D] further identify screen-induced synesthesia and cue-dependent behavior – cross-modal anchors preserved by disrupted synaptic pruning during audiovisual hyperstimulation – as additional contributors to ASD misdiagnosis in this population (Manolova & Vezenkov, 2025b; Vezenkov & Manolova, 2025b, 2026).
Critically, this framework carries clinical implications beyond etiology. In cohorts treated for screen addiction and screen trauma at the Vezenkov Center for Applied Neuroscience, children formally meeting ASD criteria showed resolution of the clinical picture following comprehensive therapy; in documented cases, the ASD diagnosis was lifted (Ivanova et al., 2025; Stefanova et al., 2025) [Grade D]. The reversibility finding distinguishes screen-induced ASD-like presentations from primary neurodevelopmental disorder, and underscores the diagnostic significance of detailed screen exposure history in early-presenting cases.
6.2.4 Short-Form Algorithmically Served Video
A meta-analysis in Psychological Bulletin (2025) examined associations between short-form video platform use and psychological outcomes across the available study base, finding consistent associations with attention deficits, anxiety, and depression in adolescents [Grade B]. Gao et al. (2025) [Grade C] used neuroimaging to characterize the neuroanatomical and functional substrates of short video addiction, finding reduced gray matter volume in prefrontal cortex and altered default-mode-network–executive-control-network coupling, with patterns consistent with broader behavioral-addiction signatures (Koob & Volkow, 2016; Volkow et al., 2019). Du et al. (2025) [Grade C] used EEG to demonstrate that algorithmically curated polarizing short-form content produced measurable disruptions in prefrontal–parietal coherence.
The design features distinguishing algorithmic short-form video from prior screen content categories – personalization calibrated to maximize individual engagement, infinite scroll, autoplay, and variable reward — collectively constitute what the behavioral pharmacology literature identifies as the engagement architecture most strongly associated with compulsive use (Koob & Volkow, 2016).
6.2.5 AI Companion Devices
AI companion devices represent an emerging high-concern category combining synthetic social contingency, personalization, and attachment-like engagement. Common Sense Media (2026) and PIRG (2025) [Grade E] have documented three categories of risk: parasocial bonding dynamics that may displace social-friction-based developmental learning; generation of age-inappropriate content despite stated safety filters in independent testing; and varying data-collection practices. The developmental risk of AI companion exposure is plausible and increasingly recognized in policy guidance (notably the UK 2026 under-5 guidance; GOV.UK, 2026), but longitudinal evidence remains limited. The framework hypothesis – that AI companions may produce attachment-system disruption at lower exposure thresholds than passive video, by occupying the attachment channel directly – is consistent with the developmental-neuroscience framework outlined by Vezenkov and Manolova (2026) [Grade D] and warrants prospective study (Vezenkov & Manolova, 2026).
6.3 Device Type and Sensory Affordances
6.3.1 Background Television
Background television – a screen active in the child's environment during activities not directed at it – has been consistently associated with negative developmental outcomes through a mechanism that does not require direct attention from the child: disruption of caregiver verbal interaction. Pempek et al. (2014) [Grade C] documented this through observational research (Anderson & Pempek, 2005; Pempek et al., 2014); Tomopoulos et al. (2010) [Grade C] linked background television exposure at 6 and 18 months to delayed language and cognitive development at 14 months (Tomopoulos et al., 2010). The EDEN birth-cohort study (n>1,700) [Grade B] documented dose-dependent negative associations between background TV and language outcomes at ages 2 and 5. The Cambridge Journal of Child Language (2025) replicated this pattern in a Saudi Arabian sample [Grade C], confirming that the mechanism is not culture-specific (Keşşafoğlu et al., 2025).
6.3.2 Touch-Screen Devices and Phonological Memory
Reshetnikova et al. (2021) [Grade C] found that passive touch-screen use was negatively associated with phonological memory in children aged 5–6, while interactive use was not — consistent with the interactivity and design-features axes of the EST/HST distinction (Section 3.3), although the study did not directly assess autonomic or cortical signatures. Brushe et al. (2024) [Grade B] used objective LENA language measurement (rather than self-report) in children aged 12–36 months and found that higher screen time was associated with fewer adult words, fewer child vocalizations, and fewer conversational turns per hour, dose-dependently (Brushe et al., 2024).
6.3.3 White Matter Integrity and Language Development
Hutton et al. (2020) [Grade C] used diffusion tensor imaging in preschool-aged children and found that higher screen use was associated with lower fractional anisotropy and axial diffusivity in white matter tracts supporting language and emergent literacy (superior longitudinal fasciculus, posterior thalamic radiation) – providing a structural neuroimaging bridge between behavioral language delay and underlying brain organization (Hutton et al., 2020). Sundqvist et al. (2024) [Grade B] in a longitudinal study found predictive negative associations between earlier screen exposure and later vocabulary, controlling for prior vocabulary (Sundqvist et al., 2024).
6.3.4 Inhibitory Control
Uzundağ et al. (2026) [Grade B], in a longitudinal study from infancy to toddlerhood, found that both background TV and overall screen exposure during 12–24 months were associated with poorer inhibitory control at toddlerhood, controlling for prior inhibitory control and temperament (Uzundağ et al., 2026). Uzundağ et al. (2022) [Grade C] previously documented cross-sectional associations between early childhood screen exposure and self-regulation difficulties (Uzundağ et al., 2022).
6.4 Social Context and Caregiver Involvement
6.4.1 The Video Deficit Effect
Anderson and Pempek (2005) [Grade B] first systematically characterized the video deficit effect — that young children learn less efficiently from screen-presented instruction than from equivalent live instruction (Anderson & Pempek, 2005). Strouse and Samson (2021) [Grade B], in the most comprehensive meta-analysis to date, found the effect robust across content domains and age groups from birth to age six, with effect sizes largest under age two (Strouse & Samson, 2021). Kuhl et al. (2003) [Grade A] demonstrated experimentally that infants learned phonemes from live social exposure but not from identical pre-recorded audiovisual presentation, establishing the social contingency hypothesis with high methodological precision (Kuhl et al., 2003).
6.4.2 Active Co-Viewing and Its Limits
Mallawaarachchi et al. (2024) [Grade B] found that caregiver co-use with active conversation was positively associated with cognitive outcomes, in contrast to negative associations for other exposure contexts (Mallawaarachchi et al., 2024). Mustonen et al. (2022) [Grade C] documented that co-viewing with active verbal interaction partially attenuated language delays (Mustonen et al., 2022). Carozza and Leong (2021) distinguish three sub-types – passive co-presence, non-interactive co-viewing, and active co-engagement – with only the third reliably attenuating negative associations (Carozza & Leong, 2021).
6.4.3 Technoference
McDaniel and Radesky (2018) [Grade C] documented associations between parental technoference and child externalizing/internalizing problems (McDaniel & Radesky, 2018). McDaniel et al. (2026) [Grade B], in a longitudinal infant study, found that caregiver use of screens to calm infants meaningfully predicted reduced emotional regulatory capacity at follow-up (McDaniel et al., 2026). Coyne et al. (2023) [Grade B] reached convergent conclusions for media-based emotion regulation in early childhood (Coyne et al., 2023). Ventura and Teitelbaum (2017) found that 92% of mothers reported personal screen device use during breastfeeding [Grade C] – a striking observation given that breastfeeding constitutes one of the densest concentrations of face-gazing, vocalization, and tactile co-regulation in the infant's experience (Ventura & Teitelbaum, 2017).
6.5 Time of Day
6.5.1 Sleep Displacement and Circadian Disruption
Beyens and Nathanson (2019) [Grade B] reported that evening electronic media use in preschool children was associated with later bedtimes, later wake times, and shorter total sleep duration, even after controlling for daytime media exposure (Beyens & Nathanson, 2019). Broader pediatric sleep literature has proposed several mechanisms linking screen exposure to sleep disruption, including displacement of sleep time, increased physiological or psychological arousal, and circadian disruption caused by evening light exposure and melatonin suppression (Hale et al., 2018) [Grade B]. In the Japanese Environment and Children’s Study (JECS), Nishioka et al. (2022) found that greater screen viewing time in children aged 1 and 3 years was associated with shorter sleep duration and later bedtimes, although the study did not directly measure cortisol or melatonin levels (Nishioka et al., 2022) [Grade B]. A Japanese study by Mineshita et al. (2021) [Grade C] further suggested that screen exposure immediately before bedtime may have adverse effects independent of total daily screen duration, emphasizing that the timing of media use may be particularly relevant for children’s sleep outcomes (Mineshita et al., 2021).
6.5.2 Moderation by Effortful Control
Clifford et al. (2020) [Grade B], in an NICHD-funded study using objective actigraphy-based sleep assessment, found that the association between pre-sleep electronic media use and poorer sleep outcomes was significantly stronger in children with lower effortful control. Children with reduced self-regulatory capacity showed greater reductions in sleep duration and sleep efficiency following bedtime media exposure, whereas the association was attenuated in children with higher effortful control (Clifford et al., 2020). These findings suggest that impaired self-regulation may increase vulnerability to the sleep-disrupting effects of evening screen exposure.
6.5.3 Clinical Trial Evidence
The ongoing SCREENS clinical trial (NCT06192745) at Baylor College of Medicine is designed to experimentally disentangle the effects of evening screen light intensity and media content arousal on children’s sleep, circadian physiology, executive functioning, and emotion regulation in children aged 8–11 years. Using a randomized factorial design comparing bright versus dim screen light and exciting versus calming content, the study is expected to provide important causal evidence regarding the mechanisms through which pre-sleep screen exposure affects pediatric sleep and circadian regulation once results become available.
6.6 Degree of Interactivity
6.6.1 Passive Versus Interactive
Veraksa et al. (2021) [Grade C] compared passive television viewing with active digital game use in preschool children and reported differential associations with phonological memory performance, suggesting that different forms of screen engagement may not have equivalent developmental effects. More recent developmental media literature has similarly argued that the psychological impact of screen exposure cannot be understood solely in terms of duration, because media activities differ substantially in their sensory stimulation, attentional demands, emotional salience, and reinforcement structure (Nustad & Abrahamsson, 2026; Veraksa et al., 2021).
A critical distinction, however, must be made between the degree of interactivity and the engagement architecture of the platform itself. An application may be formally interactive (requiring taps, swipes, rapid responses, or continuous user input) while simultaneously incorporating the defining characteristics of Hedonic Screen Time (HST), including variable reward schedules, algorithmic personalization, infinite content delivery, social reinforcement systems, progression mechanics, and the absence of natural stopping cues. Many contemporary children's games and digital platforms are therefore interactive in form but hedonic and compulsive in behavioral architecture. Under the operational framework of Section 3.3, the relevant marker is not whether the user is tapping the screen but whether the engagement produces the autonomic dominance, cortical-activation reduction, and dopaminergic engagement that define the HST neurophysiological signature.
This distinction is clinically important because interactivity alone does not determine developmental impact. Highly interactive digital environments may either support adaptive cognitive engagement or, conversely, amplify reward-seeking, compulsive use, emotional dysregulation, and prolonged attentional capture depending on their underlying reinforcement structure (Alsheail et al., 2023).
6.6.2 Algorithmically Personalized Engagement: Neurological Evidence
Zivan et al. (2019) [Grade C] used EEG in typically developing preschool children and compared six weeks of screen-based story listening with live interactive storytelling. The screen-exposure group did not show the same improvement in visual attention observed in the storytelling group and showed higher theta-versus-beta EEG connectivity patterns previously associated with attention difficulties. Parent-reported attention-difficulty scores were also related to these EEG patterns, although the study does not establish long-term clinical outcomes or screen addiction mechanisms (Zivan et al., 2019).
Gao et al. (2025) [Grade C] extended this line of evidence to short-video addiction, reporting that higher short-video addiction symptoms were associated with increased gray matter volume in the orbitofrontal cortex and bilateral cerebellum, as well as heightened spontaneous activity in the dorsolateral prefrontal cortex, posterior cingulate cortex, cerebellum, and temporal pole. Because the study was conducted in a non-clinical population and is correlational, these findings should be interpreted as neuroanatomical and functional correlates of short-video addiction symptoms rather than proof of causal brain alteration (Gao et al., 2025).
Du et al. (2025) [Grade C], used EEG, behavioral signals, and self-report measures to examine the effects of polarized short-video content. The study found that one week of exposure to polarized content produced measurable differences in emotional state, sentiment judgments, and EEG-based brain responses during subsequent video perception. These findings support the view that short-form video effects depend not only on duration but also on the affective and polarizing properties of the content itself (Du et al., 2025).
Vezenkov and Manolova (Vezenkov & Manolova, 2025c, 2026) [Grade D], drawing on several hundred qEEG and HRV recordings in screen-addicted children, adolescents, and adults, describe four classes of biomarkers that consistently appear with intensive algorithmic and video-based exposure: (1) cortical splitting — coexisting theta/alpha slowing in frontal and central leads alongside SMR/beta bursts in central, parietal, and occipital leads, convergent with the theta-versus-beta pattern reported by Zivan et al. (2019) and Vezenkov and Manolova (2025); (2) reversed hemispheric asymmetry, with dominant slow-wave activity in the left hemisphere; (3) functional fragmentation, where adjacent cortical sites operate at dominant frequencies differing by more than 1.5 Hz, with high local but weak long-range coherence; and (4) autonomic dysregulation on HRV – sympathicotonia, dorsal vagotonia, or unstable mixed patterns. High-amplitude alpha in the left occipital lead (O1) is a repeatedly observed specific marker, including in children (M. K. Swingle, 2019; Vezenkov & Manolova, 2025c) [Grade D]. A practice-derived age-linked signature is also reported: onset of intensive exposure before 18 months is associated with dominant cortical peaks at 2–3 Hz; 18–30 months with 3–4 Hz; 30–36 months with 4–5 Hz — a developmental "freezing" of the normative one-hertz-per-year frequency progression (Freschl et al., 2022; C. L. Wilkinson et al., 2024).
To operationalize state-dependence, Manolova and Vezenkov [Grade D] developed a qEEG-derived Screen Reactivity Index that quantifies the magnitude of the cortical shift from eyes-open baseline into video viewing. Two clinically distinct response profiles emerge. Before intervention, exposure typically activates a Burnout Response – a fatigued, high-theta brain pattern. After successful detox and therapy, the same exposure may instead trigger a Trance Response – rapid prefrontal slowing or dissociation in a brain that has become more, not less, reactive to screen re-exposure (Manolova & Vezenkov, 2025a). This biphasic shift demonstrates that the neurophysiological effects of algorithmic and video content are state-dependent and measurable, and that recovery does not produce screen tolerance – a finding directly relevant to policy assumptions that gradual reintroduction is safe (Petrova et al., 2025) [Grade D].
6.6.3 Game Transfer Phenomenon and Cross-Modal Anchoring
Ortiz de Gortari and Griffiths (2014) documented the Game Transfer Phenomenon (GTP) as a set of post-play experiences in which video-game-related thoughts, sensations, impulses, mental replays, perceptual distortions, and voluntary or involuntary behaviors are carried into everyday contexts [Grade D]. In their online self-report study, gamers described responding to real-life stimuli as if they were still within the game environment, including automatic thoughts, impulses, overreactions, avoidance behaviors, and involuntary movements. These experiences were interpreted as unintended after-effects of intensive game exposure and appeared to be facilitated by virtual embodiment, repetitive manipulation of game controls, and gaming habits (Ortiz De Gortari & Gackenbach, 2021; Ortiz de Gortari & Griffiths, 2014) [Grade D]. Within the present framework, GTP is treated as conceptually adjacent to screen-induced synesthesia and cue-dependent behaviors described by Manolova and Vezenkov (2025a), rather than as direct evidence for the same mechanism. Manolova and Vezenkov describe screen-induced synesthetic and cue-dependent patterns as persistent cross-modal associations and rigid behavioral dependencies linked to overstimulation-dominance of audiovisual pathways and reduced cognitive flexibility.
Vezenkov and Manolova’s proposed cross-modal anchoring model extends this literature by hypothesizing that intensive, repetitive, and emotionally salient screen exposure during sensitive developmental windows may stabilize maladaptive audiovisual, visuomotor, and cue–dependent behavior associations. This hypothesis is consistent with broader synesthesia literature suggesting that atypical persistence of cross-modal connectivity may arise from reduced developmental pruning or reduced inhibition of early cross-sensory connections, but this mechanism has not yet been directly demonstrated for GTP or screen addiction (Manolova & Vezenkov, 2025b, 2025f, 2025d).
7. Clinical Exception: Screen Addiction, Screen Trauma, and Reversed Development
7.1 Scope and Evidence Status
This section presents the clinical framework that distinguishes a specific subgroup of children for whom the population-level recommendations of Section 8 do not apply. The framework is derived from the work of the Vezenkov Center for Applied Neuroscience and synthesized in Vezenkov and Manolova (2026) and across the first volume of Nootism. We state at the outset: the clinical evidence for this framework is principally Grade D — clinical cohorts and case-series evidence supplemented by quantitative neurophysiological assessment (qEEG, HRV) — supported by convergent Grade A–C evidence from the broader neuroscience and developmental literatures. Independent prospective replication, blinded assessment, and randomized treatment comparisons remain priorities for future research and are addressed in Section 9. We present the framework here because (a) its clinical implications for the affected population are immediate; (b) its convergence with the broader neuroscience literature is substantial; and (c) policy frameworks that ignore this subgroup will inevitably misclassify and mismanage their needs.
7.2 Screen Addiction Is Not Heavy Screen Use
In the clinical model proposed by Vezenkov and Manolova (2026), severe early screen addiction is defined by four convergent clinical features (Vezenkov & Manolova, 2026) [Grade D]:
-
Compulsive seeking of high-intensity, low-social-density sensory stimulation
-
Cycles of soothing followed by dysregulation
-
Shift of interest from human faces toward objects, colors, shapes, and repetitive sensory patterns
-
Collapse of joint attention and eye-to-eye interaction
These features are not indexed by hours of exposure. A child who uses screens heavily but tolerates removal without withdrawal, maintains joint attention, and shows interest in human faces is not screen-addicted in this clinical sense. A child who meets the four criteria may be severely addicted at relatively moderate measured hours.
7.3 The Wakefulness/Dream-State Distinction and the Three Learning Systems
Vezenkov and Manolova (2026) describe two modes of cortical functioning: wakefulness – cortical readiness for human connection, serve-and-return exchange, and shared meaning – and dream-state – automatisms, immediate reward, and repetitive sensory capture. Screens can pull children into dream-state with extraordinary efficiency through fast rhythm, high contrast, instant reward, no requirement to track a face, and no ambiguity to manage (Vezenkov & Manolova, 2026).
The framework draws on three learning systems whose interaction is disrupted in screen-dominant early development. System 2 — the slow system of language, reflection, social context, and delayed action (Kahneman, 2011; Kahneman & Tversky, 1984) – matures slowly and depends on socially embedded experience. System 1 – the fast system of automatisms, immediate reward, and dopaminergic reinforcement – is exploited by the variable-reward architecture of algorithmic platforms (Koob, 2013; Koob & Volkow, 2016; Volkow et al., 2019). System 0 — the mirror neuron system bridging "I see" and "I do" (Galli et al., 2025; Rizzolatti & Craighero, 2004; Rizzolatti & Sinigaglia, 2016) – is, in screen-dominant early development, retuned away from human faces and toward 2D, accelerated, edited input. In severe early screen addiction, System 1 wins early, System 2 stalls, and System 0 is redirected – producing the social orientation profile clinically observed in this cohort (Hamilton, 2013; Vezenkov & Manolova, 2026).
7.4 The Matryoshka Hierarchy and Substitution of the Safety Source
Drawing on Hughlings Jackson (1884), Vezenkov and Manolova (2026) describe regulatory functioning as a hierarchy of nested layers from enteral regulation through phylogenetically older survival systems (fight, flight, freeze) to ventral vagal social engagement (Porges, 2021) and higher cortical regulation (Jackson, 1884; Vezenkov & Manolova, 2026). When a screen is repeatedly used to calm a distressed child, substitution of the safety source occurs: soothing shifts from the human partner to the object. Over time, reactive pathways are strengthened, so that even minimal stress shifts the child rapidly into sympathetic explosion (motor restlessness, aggression) or dorsal vagal withdrawal (vacant stare, freeze, shutdown). Screens, in the addiction context, can train the nervous system away from ventral vagal social engagement and toward older survival states (Coyne et al., 2023; Manolova & Vezenkov, 2025f; Vezenkov & Manolova, 2026).
7.5 Screen Trauma: Why Detox Alone Is Insufficient
Screen trauma refers to the durable retuning of regulatory and sensory systems such that even after screens are removed, the child remains anchored in infantile, sensory-dominant, dysregulated modes of functioning (Manolova & Vezenkov, 2025d, 2025f; Vezenkov & Manolova, 2026). What persists are developmental anchors: screen-induced pathological reflexes, vestibular and postural distortions, sensory disintegration, cortical fragmentation, and vision-dominant processing that continue to pull development backward under load. In clinical practice, the re-introduction of screens after months of detox — sometimes 30–60 minutes of video exposure — has been observed to undo months of therapeutic progress, returning the child to an ASD-like profile (Petrova et al., 2025) [Grade D].
7.6 Screen-Induced Pathological Reflexes: SIPVR and SIPECR
The Screen-Induced Pathological Vestibular Reflex (SIPVR) is elicited by a controlled backward tilt or inversion: an affected child responds with arching, frantic grasping, trembling, whole-body rigidity, and intense fear of falling – disproportionate to the postural challenge – resolving only when visual or tactile anchoring is restored (Vezenkov & Manolova, 2025e, 2025d, 2026). SIPVR is interpreted as evidence that balance, safety, and sensory integration have been pathologically reorganized with visual dominance over vestibular processing.
The Screen-Induced Pathological Eye-Covering Reflex (SIPECR) is elicited by briefly covering the child's eyes: affected children respond with immediate intense panic, screaming, agitation, and sometimes aggression toward caregivers or self-injury. SIPECR was observed in 275 of 285 children evaluated at the Vezenkov Center (96.5%) [Grade D]. Unlike a startle reflex, it is provoked by removal of visual stimulation, not its onset; unlike nyctophobia, it persists under translucent cloth in a caregiver's presence, demonstrating that the trigger is loss of familiar visual cues, not darkness (Vezenkov & Manolova, 2025d). Both reflexes resolve with therapy, supporting their environmental origin and reinforcing the clinical hypothesis of screen-induced sensory reorganization rather than primary neurological impairment.
7.7 Sensory Disintegration, Induced Synesthesia, and Cue-Dependent Behavior
Vezenkov and Manolova (2025) distinguish the screen-induced phenotype from primary sensory impairment through the concept of sensory disintegration, contrasted with sensory deprivation. In early blindness, the brain compensates by re-weighting toward vestibular and proprioceptive channels; in screen-induced ASD-like states, pathological visual dominance ("2D-locked" vision) actively suppresses these channels – explaining why SIPVR and SIPECR appear in screen addiction but not in early blindness (Vezenkov & Manolova, 2025f).
Disrupted synaptic pruning during periods of audiovisual hyperstimulation can produce screen-induced synesthesia and cue-dependent behavior (Manolova & Vezenkov, 2025b). A child may sweat on seeing a dog, perceive a parent as colored and avoid people of that color, eat only with a particular cartoon visible, defecate only when seeing a yellow image, or fall asleep only with a specific song [Grade D]. Cue-dependent behavior is a neurological inability to initiate a program without its acquired sensory key – distinguishable from ASD rigidity and amenable to dissolution through sequential therapy.
7.8 Cortical Fragmentation and "Two Ages in One Body"
The qEEG and HRV profiles of children with severe early screen addiction observed at the Vezenkov Center display four classes of biomarkers (Vezenkov & Manolova, 2025c, 2026) [Grade D]: cortical splitting (opposing activation directions across networks); reversed hemispheric asymmetry (dominant slow-wave activity in the left hemisphere); functional fragmentation (different cortical sites at different dominant frequencies, with high local but low long-range coherence); and autonomic dysregulation (sympathicotonia, dorsal vagotonia, or unstable mixed HRV).
These produce the clinical picture described as "two ages in one body": a child who solves a complex puzzle yet cannot wait a turn, recites scripts yet cannot ask for water, sits calmly with a tablet yet resists the table. External convergent evidence supports components of this profile: Law et al. (2023) [Grade C] reported that higher screen use at 12 months was associated with altered cortical EEG activity at 18 months, particularly increased relative theta power and theta/beta ratio in frontocentral and parietal regions, which partially mediated later attention and executive-function outcomes (Law et al., 2023b). Swingle [Grade B] documented atypical EEG power and connectivity in ASD and ADHD (M. K. Swingle, 2019; M. K. Swingle & Swingle, 2016; P. G. Swingle, 2002); Bellato et al. (2022) [Grade B] documented HRV-indexed autonomic arousal differences in autism and ADHD, with autistic children showing hyper-arousal during active task demands and children with ADHD showing hypo-arousal during resting-state and passive conditions (Bellato et al., 2022).
7.9 Reversed Development
Reversed development describes a condition in which evolutionarily older survival programs come to dominate higher human regulatory systems – not as fate, but as adaptive strategy in an overwhelming environment (Manolova & Vezenkov, 2025f; Vezenkov & Manolova, 2026). Clinical markers include stereotyped movements (hand-flapping, spinning, toe-walking), rigid ritualism, withdrawal of gaze from people toward objects, phylogenetically older postural patterns, and in some cases absence of nystagmus during rotation (Ornitz, 1974). The homeostasis these produce is paradoxically advantageous in the short term – radically lowering environmental complexity – which is why some parents describe affected children as having "superpowers" (rare illness, extraordinary visual recall, remarkable narrow consistency).
In clinical cohorts described by Vezenkov and Manolova, some children presenting with ASD-like, ADHD-like, or ODD-like features no longer met the same diagnostic criteria after treatment targeting screen addiction and screen trauma (Ivanova et al., 2025; Stefanova et al., 2025; Vezenkov & Manolova, 2025b) [Grade D]. These observations support the hypothesis of a screen-induced neurodevelopmental phenotype in a subgroup of children currently receiving primary neurodevelopmental diagnoses, and require prospective validation in independent cohorts. We do not claim that all ASD or ADHD presentations are screen-induced; we propose, consistent with the available clinical evidence, that screen-induced phenotypes may contribute to diagnostic confusion in a subgroup of cases.
7.10 The Nootism Therapeutic Pathway
The Nootism therapeutic framework (Vezenkov & Manolova, 2025b, 2026) describes a sequential approach corresponding to the matryoshka regulatory hierarchy: intervention must begin where the nervous system is currently operating, not where it should ideally be. The phases are:
-
Containment of defensive circuits — therapist and parent develop the capacity to hold the child's dysregulation without escalation or capitulation
-
Sequential lifting of developmental anchors — graduated SIPVR/SIPECR resolution; dissolution of induced synesthesias and cue-dependent behaviors via systematic substitution and progressive withdrawal
-
Sensory restart and cortical awakening — multisensory re-engagement reactivating the cortex through human co-regulation rather than screen-mediated stimulation
-
Reconnection and language development — language work focused on social-pragmatic embedding of words within shared human context (Mateev et al., 2025)
-
Maintenance and prevention — ongoing monitoring; HRV biofeedback and neurofeedback support consolidation
Two principles warrant emphasis: in the Nootism clinical experience, sustained recovery has not been observed when the parental screen environment remains unchanged, making parallel parental assessment and intervention a core component of the therapeutic pathway (Manolova & Vezenkov, 2025c; Pashina et al., 2025; Petrov, Manolova, et al., 2025); and re-introduction of screens after recovery has been observed to precipitate regression, indicating that the old neural pathway is not eliminated but sub-dominant, and that recovery requires sustained environmental change (Petrova et al., 2025).
7.11 Limitations of the Clinical Evidence
The clinical framework presented here is clinically coherent and biomarker-informed, but remains primarily derived from specialized clinical cohorts at the Vezenkov Center for Applied Neuroscience and a developing clinical literature in Nootism. Prevalence estimates, generalized causal claims about misdiagnosis rates, and specific recovery proportions cannot at this time be made with confidence outside the clinical-cohort context. Independent replication, prospective cohort validation, blinded assessment, randomized or quasi-experimental treatment comparisons, and population-based prevalence studies are required. These priorities are addressed explicitly in Section 9.
Box 7.1 – Clinical Red Flags for Screen Addiction or Screen Trauma
Children with the following profile warrant clinical assessment for screen addiction or screen trauma rather than primary neurodevelopmental diagnosis:
-
Screen required for feeding, sleeping, calming, or transitions
-
Withdrawal (crying, hysteria, aggression, shutdown) on device removal
-
Loss of joint attention; preference for objects, colors, or patterns over faces
-
Cue-dependent eating, defecation, or sleeping
-
Panic during eye covering (suspect SIPECR)
-
Panic or rigidity during inversion or backward tilt (suspect SIPVR)
-
ASD-like, ADHD-like, or ODD-like presentation with documented intensive early screen exposure
-
Rich verbal output (echolalia, scripting) without functional language for requesting or sharing
-
Regression following any screen re-exposure after a period of detox
-
Abnormal qEEG (cortical splitting, reversed asymmetry, fragmentation) or HRV (sympathicotonia, dorsal vagotonia) profile
-
Parental screen addiction in the household
8. Recommendations
8.1 Population-Differentiated Framework
Population differentiation is essential. The recommendations appropriate for a neurotypically developing child without prior screen-addiction history are not appropriate for a child in whom screen addiction or screen trauma has formed. We organize the recommendations around five categories of child status in Table 4:
Table 4. Child Status and Recommendations
|
Child status |
Recommendation logic |
|
No screen-addiction history, low risk |
Prevention + EST limitation + HST restriction by age |
|
High-risk household (parental screen addiction, low SES, single caregiver) but no clinical syndrome |
Stricter prevention + family-system intervention |
|
Established screen addiction or screen trauma |
No generic time limits; clinical detox and treatment pathway |
|
Post-treatment recovery |
No re-introduction unless biomarkers and clinical markers normalize and family environment is sustained |
|
Regression after re-exposure |
Full clinical reassessment; return to detox |
Sections 8.2–8.4 address Population A (no addiction history); Section 8.5 addresses Population B (established addiction or trauma); Sections 8.6–8.7 address schools and policymakers, applicable across populations.
8.2 Recommendations for Families: Ages 0–9
Ages 0–3: No Screen Exposure
No screen exposure of any kind is recommended from birth through completion of the third year. This applies without exception to passive viewing, background television, touch-screen devices, voice-interactive AI companions, and any other screen-mediated content delivery – and equally to use of screens as pacifiers, feeding aids, or calming tools during transitions. The first three years constitute the period of most intense synaptogenesis, primary language acquisition, and attachment formation (de Faria et al., 2021); the most severe and least reversible screen-addiction cases observed clinically involve onset before 18 months (Petrov, et al., 2025). We support and extend WHO (2019) guidance through the completion of the third year, in alignment with French regulatory implementation in early childhood settings (Ministère du Travail, de la Santé, des Solidarités et des Familles, 2025).
Ages 3–9: Zero as Default; Limited Euthymic Exceptions
Screen exposure is not developmentally necessary in this age range, and there is no peer-reviewed evidence of benefits unobtainable through embodied alternatives. Zero screen use is recommended as the default. HST and EST are not recommended at any dose for this age range; AI companion devices are not recommended at any dose for this age range. The recommendation does not apply to medically necessary assistive technologies or brief, caregiver-mediated live video communication where the interaction is human-contingent, non-hedonic, and not used for soothing, feeding, or sleep.
8.3 Recommendations for Families: Ages 9–18
Ages 9–12: Gradual, Supervised EST Introduction
A gradual, accompanied introduction of EST may begin after age nine:
-
EST: up to 2 hours per week total, distributed across non-consecutive days, no more than 60 minutes per single sitting, in adult presence
-
HST, Social media, gaming with variable reward, short-form video, AI companions: not recommended at any dose
Ages 12–18: Limited EST, Restricted HST, Social Media Minimum Age 16
-
EST: up to 5 hours per week, no more than 60 minutes on any single day, and a minimum of 2 days of "digital fasting".
-
Social media: minimum age 16, consistent with the legislative direction of Australia, France, Spain, and the EU regulatory trajectory. Where parental permission for limited supervised communication-platform use is granted between ages 13 and 16, it should apply to messaging applications without algorithmic feed architecture
-
Gaming: non-variable-reward formats only (chess, educational games, bounded single-player games) under 2 hours per week.
8.4 Cross-Cutting Family Principles
Measure weekly, not daily. Daily measurement creates rigid schedules that themselves become ritualized.
At least two screen-free days per week, kept flexible to prevent ritualization of the screen-free days.
No screen use within two hours of sleep; no screens in the bedroom at night – applies across all ages above nine.
Caregivers' own screen use is part of the child's developmental environment, not a neutral background condition. Parental device use during feeding, play, bedtime, and transitions competes with serve-and-return interaction and is one of the strongest predictors of child screen exposure (McDaniel & Radesky, 2018).
Recreational screen access should be framed as a developmentally regulated exposure, not as an assumed entitlement. Households in which adults hold this framing consistently report shorter and less intense daily access conflicts.
8.5 Recommendations for Children with Established Screen Addiction or Screen Trauma
The recommendations in 8.2–8.4 apply to children whose nervous systems have not been reorganized around screen-induced dysregulation. They are not appropriate for children in whom early screen addiction, screen trauma, or reversed development has formed. For these children, generic time-limit guidance does not apply and may be actively misleading by implying that gradual exposure reduction is safe.
The recommendations for this population constitute a clinical pathway, not a behavioral guideline.
8.5.1 Objective Clinical Assessment
Comprehensive assessment is the necessary first step:
-
qEEG with Screen Reactivity Index (Manolova & Vezenkov, 2025a)
-
HRV and autonomic nervous system assessment
-
SIPVR and SIPECR screening (Vezenkov & Manolova, 2025e, 2025d)
-
Developmental and behavioral evaluation including language assessment, joint attention, induced synesthesia inventory, cue-dependent behavior inventory (Manolova & Vezenkov, 2025b)
-
Parental qEEG and HRV assessment, screening for parental screen addiction and family-system dynamics (Manolova et al., 2025; Manolova & Vezenkov, 2025c; Pashina et al., 2025; Petrov, Manolova, et al., 2025; Vezenkov & Manolova, 2025a)
8.5.2 Complete Digital Detox
Complete digital detox — total elimination of all screen and digital device exposure including background television, parental device use in the child's presence, AI companion devices, and incidental exposure in public or educational settings – is necessary but not sufficient: detox removes the stimulus but leaves the developmental anchors and state-dependent behavioral patterns (Vezenkov & Manolova, 2026).
For severe early-onset cases – onset before 36 months, positive SIPVR/SIPECR, full ASD-like or ADHD-like presentation, abnormal qEEG/HRV – the Nootism clinical pathway recommends complete digital detox of a minimum of two years before any consideration of re-exposure. This recommendation is clinical and biomarker-guided, not a population-level guideline. For less severe cases, the duration is individually calibrated by biomarker normalization and clinical assessment of developmental anchor resolution. Abrupt detox without concurrent therapeutic support is contraindicated; detox and therapy must begin concurrently.
8.5.3 The Nootism Therapeutic Pathway
The five sequential phases (Section 7.10) – containment of defensive circuits → lifting of developmental anchors → sensory restart and cortical awakening → reconnection and language development → maintenance – must be addressed in order, with each phase providing the regulatory foundation for the next.
8.5.4 Parallel Therapeutic Work with Parents
In the Nootism clinical experience, sustained child recovery has not been observed when the parental screen environment remains unchanged (Manolova et al., 2025; Manolova & Vezenkov, 2025c; Pashina et al., 2025; Petrov, Manolova, et al., 2025; Vezenkov & Manolova, 2026). This is a clinical requirement: parental therapeutic work includes assessment for parental screen addiction (gaming, pornography, social media, gambling) with treatment where indicated; individual neurotherapeutic work where parental anxiety, depression, or trauma is present; couples work where indicated; and guided re-attachment work. Cases where parents are unwilling to engage in parallel work should, in the judgment of treating clinicians, be declined.
8.6 Recommendations for Schools and Educators
8.6.1 Personal Devices and School-Issued Devices
-
No personal devices (smartphones, smartwatches, internet-connected wearables) accessible bell-to-bell on school premises for under-16s, with storage-based enforcement
-
No school-issued tablets or laptops in early childhood education (under 9)
-
No screen-based homework in primary school
-
No algorithmic platforms (YouTube autoplay, social-media-style content delivery) for educational delivery under 9.
-
No AI companion devices or AI tutors in early childhood settings
-
Bell-to-bell storage architecture (lockers, locked pouches, collection at entry) — funded by the institution, not by families
-
Clear exception protocols for medical devices, disability accommodations, genuine emergencies
-
Teacher training on consistent enforcement and on recognizing screen-induced developmental presentations (Section 7)
The Los Angeles Unified model (classroom screen-time caps + school-issued device restrictions, Subtype A5) is the most appropriate template where extensive educational technology has already been deployed (Ede-Osifo, 2026).
8.6.2 Pilot Before Scaling
Any educational technology not evaluated longitudinally for both cognitive benefit and health risk should not be adopted at scale without a structured pilot phase. Finland's combination of school phone restrictions with a national longitudinal evaluation study represents the correct sequence: restrict while evaluating, rather than expand while hoping. Required pre-registered metrics: standardized academic performance, standardized mental health screening, teacher-assessed engagement, parental report of home spillover, minimum three-year evaluation horizon.
8.6.3 Educator Training in Recognizing Screen-Induced Presentations
Teacher training programs and continuing professional development should include neurodevelopmental literacy on the sensitive window model and screen-induced developmental disruption; recognition of clinical red flags (Box 7.1); and clear referral pathways to clinical services specializing in screen addiction assessment.
8.7 Recommendations for Policymakers and Public Health
8.7.1 Early Childhood Screen Exposure as a Child-Safeguarding Matter
The deliberate, sustained provision of intensive screen exposure to an infant or toddler — particularly as a substitute for human co-regulation, feeding support, or calming — is not meaningfully different in developmental consequence from other forms of caregiver-mediated environmental harm that child-protection frameworks already govern. We support the legislative direction of Taiwan (2015) and recommend that governments, at minimum, introduce a professional obligation for pediatricians and health visitors to inquire about screen exposure in families with children under three; include excessive screen exposure in the differential assessment of developmental presentations; and ensure that child protection services have standing to intervene where clinical assessment establishes moderate-to-severe environmentally-mediated developmental harm.
8.7.2 Social Media Minimum Age and Effective Age Verification
We support the establishment of 16 as the minimum age for social media account creation, consistent with Australia, Spain, France, Indonesia, and the EU trajectory. Age-verification mechanisms must be technically robust: governments should invest in interoperable, privacy-preserving infrastructure (the EU Age Verification Application and Digital Identity Wallets are the most promising technical direction) as a prerequisite to effective enforcement.
8.7.3 Platform Design Regulation as the Priority Direction
Of the six policy models, Model C is most directly targeted at the mechanism of harm. Recommendations:
-
Mandatory elimination of autoplay, infinite scroll, and variable-reward notification schedules for users under 18
-
Mandatory verified "minor mode" on smartphones and connected devices, with platform-enforced content restrictions, time caps, and night curfews
-
Prohibition of loot boxes and variable-reward in-game mechanics for users under 18
-
Prohibition of algorithmic personalization of feeds for under-18s without explicit informed parental consent
-
Platform liability for recommender systems producing compulsive use, with the burden of proof on platforms to demonstrate safety
8.7.4 Clinical Infrastructure for Screen Addiction Assessment and Treatment
-
Clinical training in screen addiction assessment and treatment (qEEG, HRV, SIPVR/SIPECR, Nootism therapeutic pathway)
-
Formal recognition of screen addiction and screen trauma as clinical diagnostic categories within national healthcare frameworks
-
Clinical referral pathways from pediatric primary care, school health services, and child protection services to specialized assessment centers
-
Multicenter longitudinal research, including randomized treatment comparisons, to build the independent evidence base
8.7.5 Parental Screen Addiction as a Child-Safeguarding Risk Factor
Parental screen use is the strongest population-level predictor of child screen exposure. Brief screening for adult screen addiction should be integrated into routine pediatric and family-health encounters; pediatricians assessing developmental or behavioral concerns should inquire about parental gaming, pornography, social media, and overall device use; positive screen → referral to adult assessment in parallel with the child's clinical management.
8.8 Extension of the Section 8.5 Framework to Other Clinically Vulnerable Populations
The clinical pathway developed in Section 8.5 was articulated in reference to children with established screen addiction or screen trauma, but its underlying logic is not specific to those etiologies. The eight-dimension framework (Section 3.2) identifies pre-existing neuroregulatory state as the dimension that determines how a given exposure is processed; where that state is already compromised, the population-level recommendations of Sections 8.2–8.4 do not apply and may be actively harmful. Several additional populations meet this criterion and should, in the clinical judgement of treating teams, be managed under the Section 8.5 framework rather than under generic age-based guidance.
8.8.1 Populations Covered by This Extension
The Section 8.5 framework applies, with the modifications outlined below, to the following groups:
Children with trauma history – including acute psychological trauma, complex developmental trauma, attachment trauma, exposure to domestic or community violence, and post-traumatic stress presentations. Trauma reorganizes autonomic regulation along the same sympathetic-hyperarousal / dorsal-vagal-shutdown axis that is disrupted in screen addiction and screen trauma (Section 7). Variable-reward and hyperstimulating screen content does not return such a child toward ventral vagal regulation; it entrenches the dysregulated state and competes with the relational repair that is the central therapeutic task.
Children with toxic stress – children subject to sustained adverse childhood experiences, chronic caregiver dysregulation, household instability, neglect, or socioeconomic adversity sufficient to produce chronic activation of the stress-response systems. The neurobiological signature of toxic stress overlaps substantially with that of screen-induced dysregulation; in many high-risk households the two compound rather than substitute, and disentangling them requires the assessment protocol described in 8.5.1.
Children with genetic syndromes presenting with "wounded" or atypical developmental trajectories – including neurogenetic conditions affecting cortical organization, sensory integration, language acquisition, attachment behavior, or autonomic tone (for example, Fragile X, tuberous sclerosis complex, Williams, Angelman, Rett, 22q11.2 deletion, and related syndromes), as well as syndromic and non-syndromic intellectual disability. For these children, the developmental anchors and state-dependent vulnerabilities described in Section 7 apply with particular force; sensitive windows are narrower, regulatory reserves are smaller, and recovery from dysregulating exposure is slower. Generic time-limit guidance is therefore an inadequate framework even where screen exposure has not previously been intensive.
Children recovering from major medical interventions – including post-surgical recovery, recovery from intensive treatment regimens (oncological, cardiac, transplant, neurological, severe burns), prolonged hospitalization, and recovery from acute illness with neurological or autonomic involvement. During recovery, the nervous system is actively engaged in re-establishing autonomic balance and supporting neuroplastic repair; intensive screen exposure during this period competes directly with the regulatory and reparative processes the child's physiology is attempting to complete.
These populations are not mutually exclusive – a child recovering from oncological treatment may also carry trauma from the treatment trajectory itself; a child with a genetic syndrome may live in a high-toxic-stress environment. Where two or more apply, the more conservative end of the Section 8.5 framework is the appropriate default.
8.8.2 Application of the Section 8.5 Pathway
For the populations identified in 8.8.1, the four components of Section 8.5 apply as follows:
Clinical assessment (8.5.1) is the entry point. Screen-exposure decisions are made on the basis of clinical assessment of regulatory state (qEEG with Screen Reactivity Index, HRV, SIPVR/SIPECR screening where indicated, developmental and behavioral evaluation) rather than on chronological age alone. The standard pediatric or specialty assessment does not substitute for this and is not designed to detect screen-mediated dysregulation in a child whose primary diagnosis lies elsewhere.
Digital detox (8.5.2) is calibrated to clinical state, not applied as an absolute two-year rule. The two-year minimum specified in 8.5.2 is reserved for severe early-onset screen-induced presentations; for the populations described here, the duration is set by biomarker normalization, by the trajectory of the underlying condition (post-surgical recovery, syndrome-specific developmental milestones, resolution of toxic stress exposures), and by clinical judgement of regulatory reserve.
The therapeutic pathway (8.5.3) is adapted to the primary condition. The five sequential phases – containment of defensive circuits, lifting of developmental anchors, sensory restart and cortical awakening, reconnection and language development, and maintenance – are integrated into, rather than substituting for, the child's primary clinical management (oncological, surgical, neurogenetic, trauma-focused, or otherwise). The ordering principle is preserved: regulatory containment precedes higher-order developmental work.
Parallel work with the family system (8.5.4) applies with equal force. Parents of medically complex, traumatized, or syndromic children carry elevated rates of anxiety, depression, exhaustion-driven device use, and dependence on screens as a calming tool for the child; these patterns are part of the recovery environment, not a neutral background condition. Family-system intervention is part of the clinical pathway, not an optional add-on.
8.8.3 Specific Guidance for Medical and Therapeutic Settings
Hospital wards, oncology day units, dialysis suites, rehabilitation centers, and outpatient therapy settings routinely use screens as a behavioral management tool – to occupy, distract, calm, or compensate for the absence of family during prolonged admissions. This practice is understandable but, in the populations identified here, is not without cost.
The following principles apply:
-
Screens used in medical or therapeutic settings should be time-limited, content-restricted, and adult-mediated, not provided as continuous default background.
-
No algorithmic feeds, no variable-reward gaming, no autoplay, no short-form video platforms in inpatient or recovery settings; defined-endpoint content (a specific film, a chosen episode, a video call with a family member) is preferable where any screen use is judged appropriate.
-
Active adult co-regulation accompanies any screen use, rather than the screen substituting for the regulating adult. Where staff capacity is the limiting factor, this is an institutional rather than a clinical problem and should be acknowledged as such.
-
Re-introduction following recovery is timed and graded in accordance with the principles set out in 8.5.2, not by reflexive return to pre-illness exposure patterns. The recovery window is itself a sensitive window; the developmental gain available during convalescence is lost if it is filled with passive screen consumption.
8.8.4 Population Framework Cross-Reference
The population categories listed in Section 8.1 should be read as including the groups described in 8.8.1 within the "established screen addiction or screen trauma" row, in the sense that the clinical pathway – not the population-level recommendations – is the appropriate framework. The mechanism of vulnerability differs (the etiology is medical, genetic, or trauma-related rather than screen-induced), but the regulatory consequence – a nervous system that cannot safely process exposures appropriate for a neurotypical, non-traumatized, medically well peer – is shared, and the clinical implication is identical.
The principle underlying this extension is that the determining variable for screen-exposure decisions is the child's neuroregulatory state, not the etiology that produced it. Where regulatory reserve is compromised, the framework that applies is the clinical pathway of Section 8.5.
9. Limitations
This article has several limitations that warrant explicit acknowledgement.
Methodology. The article is a narrative review and policy mapping rather than a systematic review; it does not apply formal PRISMA procedures or pre-registered search strategies. The complete coding table (Appendix A) is intended to make the policy mapping reproducible.
Rapidly changing policy landscape. Several policies referenced in Section 4 reflect the best information available at the May 10, 2026 cut-off. Some legislation was passed by parliament but awaiting final enactment; some was issued as ministerial guidance without binding legal force; some was announced but not implemented. Where uncertainty remains, this is noted in the text.
Reliance on government and media sources for very recent developments. Particularly for late-2025 and 2026 measures, primary statutory text was not always publicly available at the time of writing, and reliance on government press releases, intergovernmental reports, and high-reliability media sources was unavoidable. Independent verification through national legal databases would strengthen subsequent versions.
Limited causal evidence on school bans. The strongest available causal evidence comes from a single quasi-experimental study (Norway, SSRN 2025), with most other evidence cross-sectional or observational. The SMART Schools study, frequently cited in policy debates, is a multi-method cross-sectional observational study, not a randomized trial. Causal claims about school phone policies should be calibrated to this evidence base.
Self-report limitations in screen-time measurement. Most population-level evidence on screen exposure relies on parental or self-report, which substantially underestimates objective measurement (Radesky et al., 2020; Zhao et al., 2025). Objective sensor-based measurement (Vadathya et al., 2022) and ecological momentary assessment with passive smartphone monitoring (Zhao et al., 2025) are needed for robust epidemiological characterization.
Early-stage evidence for emerging exposure categories. AI companion devices, generative AI tutors, and the most recent generation of algorithmically optimized short-form video platforms have outpaced the research cycle. Recommendations for these categories rest on theoretical convergence with the established framework rather than on direct longitudinal evidence; this is acknowledged where relevant.
Clinical framework requires independent validation. The Nootism clinical framework presented in Section 7 is supported by clinical-cohort evidence and quantitative neurophysiological assessment at the Vezenkov Center, with convergent support from the broader neuroscience and developmental literatures. It has not yet been prospectively validated in independent clinical samples, with blinded assessment, against control conditions, or with treatment-comparison randomization. Prevalence estimates, generalized misclassification rates, and specific recovery proportions therefore cannot be made with confidence outside the clinical-cohort context. Section 8.7.4 calls explicitly for the research infrastructure required to address these gaps.
Precautionary policy orientation. Several recommendations in Section 8 — particularly for AI companion devices, the under-3 zero-exposure recommendation, the framing of severe early childhood screen exposure as a safeguarding matter, and the platform design regulation priorities — extend beyond what direct longitudinal evidence currently establishes, and adopt a precautionary stance grounded in convergent evidence and the irreversibility of damage in sensitive developmental windows. This precautionary orientation is explicit and is offered as a deliberate policy stance, not as a claim of definitive empirical proof.
10. Conclusion
The international policy response to child digital exposure has accelerated to an unprecedented scale: 114 education systems with national mobile-phone restrictions; an emerging consensus on under-16 social media age thresholds; binding institutional prohibitions in early childhood settings – France's national crèche ban (Model D, in force July 2025), Madrid's regional weekly screen caps, and Bulgaria's Ministry-of-Health regulation; and a developing platform design regulatory architecture under the EU Digital Services Act. These represent a major political achievement and establish, for the first time at scale, that children's digital exposure is a matter of public concern rather than purely private preference.
This achievement is necessary but not sufficient. The evidence assembled in this article supports four convergent conclusions.
First, the dominant policy metric – hours of screen time per day or per week – is conceptually inadequate. Screen interaction, defined by the intersection of content type, device and sensory affordances, interactivity, social context, time of day, motivational purpose, design architecture, and the child's regulatory state, is the appropriate unit of analysis. The euthymic versus hedonic screen time (EST/HST) distinction, neurophysiologically grounded in autonomic, cortical, and dopaminergic signatures (Manolova & Vezenkov, 2025d) and operationalized across ten behavioral, neurophysiological, and clinical criteria, makes the framework measurable in family practice, clinical assessment, and policy design (Section 3.3; Table 1).
Second, the dominant pattern of single-axis policies is displacement, not reduction, of total developmental exposure — though Norway's quasi-experimental evidence (Abrahamsson, 2024) [Grade A] demonstrates that causal positive effects are achievable under conditions of enforcement fidelity, particularly for low-SES girls. School device restrictions reliably reduce in-school use but rarely reduce total daily use without complementary home and platform measures (Goodyear et al., 2025; Reynolds et al., 2025). Social media age restrictions face structural circumvention in the absence of interoperable age-verification infrastructure; the EU Age Verification Application and Digital Identity Wallets represent the most promising technical direction. Parental adherence to existing guidelines is consistently low for structural rather than informational reasons: only 24.7 % of families with children under two meet the zero-screen recommendation (McArthur et al., 2022) [Grade B]. Implementation fidelity is a further constraint: France's ~9 % collège adoption at term start (Morin, 2025) is representative of the gap between legislative announcement and institutional implementation. Effective protection therefore requires multi-axis intervention coordinated across school, platform, family, and clinical domains.
Third, the population for whom these regulatory measures are most needed is also the population for whom they are least sufficient. A clinically distinct subgroup of children – in whom early screen exposure has produced compulsive sensory seeking, withdrawal on device removal, collapse of joint attention, and the downstream sensory and autonomic reorganization we describe as screen trauma and reversed development – requires a sequential clinical pathway rather than a behavioral guideline. The Nootism clinical framework, supported by quantitative neurophysiological assessment (qEEG, HRV, SIPVR, SIPECR) and case-series evidence from the Vezenkov Center, identifies this population through specific biomarkers and clinical reflexes (Vezenkov & Manolova, 2026) [Grade D]. Independent prospective validation in multi-center cohorts – with blinded assessment, standardized assessment protocols, and treatment-comparison designs – is the principal research priority arising from this article.
Fourth, of the six regulatory models, platform design regulation (Model C) is most directly targeted at the mechanism of harm: the autoplay, infinite scroll, variable reward, and algorithmic personalization architectures that produce compulsive engagement by design rather than by accident. A multi-axis agenda combines this with bell-to-bell school device restriction (Model A, with explicit Subtype A5 attention to school-issued tablets and laptops), early childhood institutional prohibition (Model D), time-of-day regulation (Model E) where platform-enforced curfews or default-on parental controls are politically feasible, family-system intervention to address parental screen habits, and clinical pathway access for affected children (Model F). No single component, deployed in isolation, is sufficient.
The cost of acting precautionarily on incomplete evidence, in this domain, is small compared to the cost of waiting: the population on which the developmental evidence would mature is the same population currently passing through its most sensitive developmental windows. The window for protective regulation is itself developmental.
References
Abrahamsson, S. (2024). Smartphone Bans, Student Outcomes and Mental Health (SSRN Scholarly Paper No. 4735240). Social Science Research Network. https://doi.org/10.2139/ssrn.4735240
AFP. (2026, February 2). Snapchat blocks 415,000 under-age accounts in Australia. Al Arabiya English. https://english.alarabiya.net/News/world/2026/02/02/snapchat-blocks-415000-underage-accounts-in-australia-
Albuquerque, F. (2025, September 28). Cell phone ban boosts attention in class for 80% of Brazilian students. Agência Brasil. https://agenciabrasil.ebc.com.br/en/educacao/noticia/2025-09/cell-phone-ban-boosts-attention-class-80-brazilian-students
Alsheail, M., Alexandrovskz, D., & Gerling, K. (2023). Designing for Disengagement: Challenges and Opportunities for Game Design to Support Children’s Exit From Play (arXiv:2303.15400). arXiv. https://doi.org/10.48550/arXiv.2303.15400
Anas, E. B. (2025, August 18). Belgium to enforce nationwide school ban on mobile phones this term. The Brussels Times. https://www.brusselstimes.com/1705945/belgium-to-enforce-nationwide-school-ban-on-mobile-phones-starting-this-year
Anderson, D. R., & Pempek, T. A. (2005). Television and Very Young Children. American Behavioral Scientist, 48(5), 505–522. https://doi.org/10.1177/0002764204271506
AP News. (2026, March 27). Austria plans social media ban for under-14s | AP News. https://apnews.com/article/austria-government-social-media-under-14-ban-7516559412eecd9197df70ed958186fe
Atzil, S., Gao, W., Fradkin, I., & Barrett, L. F. (2018). Growing a social brain. Nature Human Behaviour, 2(9), 624–636. https://doi.org/10.1038/s41562-018-0384-6
Baggio, S., Wade, T., Radunz, M., Galanis, C. R., Billieux, J., Starcevic, V., Quinney, B., & King, D. L. (2025). Psychological consequences of school mobile phone bans: Emulated trial of a natural experiment in South Australia. Computers in Human Behavior, 172, 108767. https://doi.org/10.1016/j.chb.2025.108767
Ballotpedia. (2026, April 10). State policies on cellphone use in K-12 public schools. Ballotpedia. https://ballotpedia.org/State_policies_on_cellphone_use_in_K-12_public_schools
Barrett, M. (2025, September 30). Denmark agrees plan to ban mobile phones from schools. The Local Denmark. https://www.thelocal.dk/20250930/denmark-agrees-plan-to-ban-mobile-phones-from-schools
Bellato, A., Arora, I., Kochhar, P., Ropar, D., Hollis, C., & Groom, M. J. (2022). Heart Rate Variability in Children and Adolescents with Autism, ADHD and Co-occurring Autism and ADHD, During Passive and Active Experimental Conditions. Journal of Autism and Developmental Disorders, 52(11), 4679–4691. https://doi.org/10.1007/s10803-021-05244-w
Beyens, I., & Nathanson, A. I. (2019). Electronic Media Use and Sleep Among Preschoolers: Evidence for Time-Shifted and Less Consolidated Sleep. Health Communication, 34(5), 537–544. https://doi.org/10.1080/10410236.2017.1422102
Braghieri, L., Levy, R., & Makarin, A. (2022). Social Media and Mental Health. American Economic Review, 112(11), 3660–3693. https://doi.org/10.1257/aer.20211218
Brushe, M. E., Haag, D. G., Melhuish, E. C., Reilly, S., & Gregory, T. (2024). Screen Time and Parent-Child Talk When Children Are Aged 12 to 36 Months. JAMA Pediatrics, 178(4), 369. https://doi.org/10.1001/jamapediatrics.2023.6790
Bryant, M. (2025, April 30). Finland restricts use of mobile phones during school day. The Guardian. https://www.theguardian.com/education/2025/apr/30/finland-restricts-use-of-mobile-phones-during-school-day
Carozza, S., & Leong, V. (2021). The Role of Affectionate Caregiver Touch in Early Neurodevelopment and Parent–Infant Interactional Synchrony. Frontiers in Neuroscience, 14. https://doi.org/10.3389/fnins.2020.613378
Champion-Osselin, Y. (2025, August 25). Screens In Classrooms? A Serious Swedish Debate Spreads Worldwide. Worldcrunch. https://worldcrunch.com/culture-society/sweden-phones-in-schools/
Chen, L. (2025, January 1). Zhengzhou the first city in China to ban cellphone use in schools. South China Morning Post. https://www.scmp.com/news/china/politics/article/3292863/zhengzhou-first-city-china-ban-cellphone-use-schools
Clifford, S., Doane, L. D., Breitenstein, R., Grimm, K. J., & Lemery-Chalfant, K. (2020). Effortful Control Moderates the Relation Between Electronic-Media Use and Objective Sleep Indicators in Childhood. Psychological Science, 31(7), 822–834. https://doi.org/10.1177/0956797620919432
Common Sense Media. (2026, January 22). AI Toys. https://www.commonsensemedia.org/ai-ratings/ai-toys
Cosseboom, L. (2026, March 8). Indonesia Social Media Ban March 2026: Impact on Brands. Mission Media. https://missionmedia.asia/indonesia-under-16-social-media-ban-march-2026/
Coyne, S. M., Rogers, A., Holmgren, H. G., Booth, M. A., Van Alfen, M., Harris, H., Barr, R., Padilla-Walker, L. M., Sheppard, J. A., Shawcroft, J., & Ober, M. (2023). Masters of media: A longitudinal study of parental media efficacy, media monitoring, and child problematic media use across early childhood in the United States. Journal of Children and Media, 17(3), 318–335. https://doi.org/10.1080/17482798.2023.2200958
de Faria, O., Pivonkova, H., Varga, B., Timmler, S., Evans, K. A., & Káradóttir, R. T. (2021). Periods of synchronized myelin changes shape brain function and plasticity. Nature Neuroscience, 24(11), 1508–1521. https://doi.org/10.1038/s41593-021-00917-2
Department of Education. (2026a, February 19). Mobile phones in schools. GOV.UK. https://www.gov.uk/government/publications/mobile-phones-in-schools/mobile-phones-in-schools
Department of Education. (2026b, March 26). New screen time guidance for parents of under-5s. GOV.UK. https://www.gov.uk/government/news/new-screen-time-guidance-for-parents-of-under-5s
Du, B., Ye, Z., Jankowska, M., Wu, Z., Ai, Q., Zhou, Y., & Liu, Y. (2025). EEG reveals the cognitive impact of polarized content in short video scenarios. Scientific Reports, 15(1), 18277. https://doi.org/10.1038/s41598-025-02423-y
Eckstein, M., Mamaev, I., Ditzen, B., & Sailer, U. (2020). Calming Effects of Touch in Human, Animal, and Robotic Interaction—Scientific State-of-the-Art and Technical Advances. Frontiers in Psychiatry, 11. https://doi.org/10.3389/fpsyt.2020.555058
Ede-Osifo, U. (2026, April 22). Los Angeles school board votes to set limits on classroom screen time. The Guardian. https://www.theguardian.com/us-news/2026/apr/22/los-angeles-school-district-screen-time
Éducaloi, A. (2025, September 4). No More Cellphones in Schools: What You Need to Know | In the News. Éducaloi. https://educaloi.qc.ca/en/legal-news/no-more-cellphones-in-schools-what-you-need-to-know/
Edward, A. (2026, April 26). How Malaysia plans to limit social media access to youngsters. Free Malaysia Today | FMT. https://www.freemalaysiatoday.com/category/nation/2026/04/27/how-malaysia-plans-to-limit-social-media-access-to-youngsters
ERO. (2025, November 20). Do not disturb: A review of removing cell phones from New Zealand’s classrooms – Summary. https://www.evidence.ero.govt.nz/documents/do-not-disturb-a-review-of-removing-cell-phones-from-new-zealand-s-classrooms-summary/
eSafety Commissioner. (2026, March). Social media age restrictions. https://www.esafety.gov.au/about-us/industry-regulation/social-media-age-restrictions
Euronews. (2024, August 31). Mobile phones to be banned in Greek schools from September. Euronews. https://www.euronews.com/my-europe/2024/08/31/greece-announces-new-rules-banning-mobile-phones-in-schools-from-september
Euronews. (2025, February 7). New law in Brazil restricts smartphones in schools. Euronews. https://www.euronews.com/next/2025/02/07/new-law-in-brazil-restricts-smartphones-in-schools
European Commission. (2025). Commission publishes guidelines on the protection of minors | Shaping Europe’s digital future. https://digital-strategy.ec.europa.eu/en/library/commission-publishes-guidelines-protection-minors
Eurydice Unit Portugal. (2025, October 27). Portugal: Prohibition of the use of mobile electronic communication devices with Internet access in primary schools. Eurydice Unit Portugal. https://eurydice.eacea.ec.europa.eu/news/portugal-prohibition-use-mobile-electronic-communication-devices-internet-access-primary
Freschl, J., Azizi, L. A., Balboa, L., Kaldy, Z., & Blaser, E. (2022). The development of peak alpha frequency from infancy to adolescence and its role in visual temporal processing: A meta-analysis. Developmental Cognitive Neuroscience, 57, 101146. https://doi.org/10.1016/j.dcn.2022.101146
Galli, J., Dusi, L., Garofalo, G., Brizzi, A., Gritti, M., Polo, F., Fazzi, E., & Buccino, G. (2025). Children with autistic spectrum disorder can imagine actions—What can this reveal about the Broken Mirror Hypothesis? Frontiers in Neurology, 16, 1490445. https://doi.org/10.3389/fneur.2025.1490445
Gao, Y., Hu, Y., Wang, J., Liu, C., Im, H., Jin, W., Zhu, W., Ge, W., Zhao, G., Yao, Q., Wang, P., Zhang, M., Niu, X., He, Q., & Wang, Q. (2025). Neuroanatomical and functional substrates of the short video addiction and its association with brain transcriptomic and cellular architecture. NeuroImage, 307, 121029. https://doi.org/10.1016/j.neuroimage.2025.121029
Goodyear, V. A., Randhawa, A., Adab, P., Al-Janabi, H., Fenton, S., Jones, K., Michail, M., Morrison, B., Patterson, P., Quinlan, J., Sitch, A., Twardochleb, R., Wade, M., & Pallan, M. (2025). School phone policies and their association with mental wellbeing, phone use, and social media use (SMART Schools): A cross-sectional observational study. The Lancet Regional Health – Europe, 51. https://doi.org/10.1016/j.lanepe.2025.101211
Groen, R. (2026, March 28). Indonesia social media ban for minors comes into effect. https://www.jurist.org/news/2026/03/indonesia-social-media-ban-for-minors-comes-into-effect/
Haidt, J. (2024). The Anxious Generation: How the Great Rewiring of Childhood Is Causing an Epidemic of Mental Illness. Penguin Press.
Hale, L., Kirschen, G. W., LeBourgeois, M. K., Gradisar, M., Garrison, M. M., Montgomery-Downs, H., Kirschen, H., McHale, S. M., Chang, A.-M., & Buxton, O. M. (2018). Youth screen media habits and sleep: Sleep-friendly screen-behavior recommendations for clinicians, educators, and parents. Child and Adolescent Psychiatric Clinics of North America, 27(2), 229–245. https://doi.org/10.1016/j.chc.2017.11.014
Hamilton, A. F. D. C. (2013). Reflecting on the mirror neuron system in autism: A systematic review of current theories. Developmental Cognitive Neuroscience, 3, 91–105. https://doi.org/10.1016/j.dcn.2012.09.008
Heffler, K. F., Acharya, B., Subedi, K., & Bennett, D. S. (2024). Early-Life Digital Media Experiences and Development of Atypical Sensory Processing. JAMA Pediatrics, 178(3), 266. https://doi.org/10.1001/jamapediatrics.2023.5923
Heffler, K. F., Frome, L. R., & Gullo, D. F. (2022). Changes in autism symptoms associated with screen exposure: Case report of two young children. Psychiatry Research Case Reports, 1(2), 100059. https://doi.org/10.1016/j.psycr.2022.100059
Heffler, K. F., Sienko, D. M., Subedi, K., McCann, K. A., & Bennett, D. S. (2020). Association of Early-Life Social and Digital Media Experiences With Development of Autism Spectrum Disorder–Like Symptoms. JAMA Pediatrics, 174(7), 690. https://doi.org/10.1001/jamapediatrics.2020.0230
Hilotin, J. (2025, October 27). Do smartphones make kids dumb? Countries that ban gadgets for students. Gulf News: Latest UAE News, Dubai News, Business, Travel News, Dubai Gold Rate, Prayer Time, Cinema. https://gulfnews.com/special-reports/do-smartphones-make-kids-and-teens-dumb-countries-that-ban-gadgets-for-students-1.500322013
Hoppe, D. B. (2020, May 27). Japanese Teen Fights Kagawa’s “Screen Time” Law—Gamma Law. https://gammalaw.com/japanese-teen-fights-kagawas-screen-time-law/
Hutton, J. S., Dudley, J., Horowitz-Kraus, T., DeWitt, T., & Holland, S. K. (2020). Associations Between Screen-Based Media Use and Brain White Matter Integrity in Preschool-Aged Children. JAMA Pediatrics, 174(1), e193869. https://doi.org/10.1001/jamapediatrics.2019.3869
Ilyka, D., Johnson, M. H., & Lloyd-Fox, S. (2021). Infant social interactions and brain development: A systematic review. Neuroscience & Biobehavioral Reviews, 130, 448–469. https://doi.org/10.1016/j.neubiorev.2021.09.001
IMDA. (2025, January 15). New Online Safety Code of Practice for App Distribution Services Enhances Protection for Singapore Users. Infocomm Media Development Authority. https://www.imda.gov.sg/resources/press-releases-factsheets-and-speeches/press-releases/2025/online-safety-code-of-practice-for-app-distribution-services
Ivanova, V., Mitsova, S., Petrova, T., Manolova, V., & Vezenkov, S. (2025). Full Recovery of a 10-Year-Old Girl with Persistent Screen Addiction Since Age 2 and Autism Spectrum Disorder: Case Report. Nootism, 1, 17–26. https://doi.org/10.64441/nootism.1.3.3
Jackson, J. H. (1884). The Croonian Lectures on Evolution and Dissolution of the Nervous System. British Medical Journal, 1(1215), 703–707. https://doi.org/10.1136/bmj.1.1215.703
Ji-hye, S. (2025, August 27). Phones banned in class starting March 2026—The Korea Herald. https://www.koreaherald.com/article/10563208
Jones, S. (2025, March 20). Madrid plans to limit computer and tablet use in primary schools to two hours a week. The Guardian. https://www.theguardian.com/world/2025/mar/20/madrid-plans-to-limit-computer-and-tablet-use-in-primary-schools-to-two-hours-a-week
Júdice, P. B., Sousa-Sá, E., & Palmeira, A. L. (2023). Discrepancies Between Self-reported and Objectively Measured Smartphone Screen Time: Before and During Lockdown. Journal of Prevention (2022), 44(3), 291–307. https://doi.org/10.1007/s10935-023-00724-4
Kahneman, D. (2011). Thinking, fast and slow. Farrar, Straus and Giroux. New York.
Kahneman, D., & Tversky, A. (1984). Choices, values, and frames. American Psychologist, 39(4), 341–350. https://doi.org/10.1037/0003-066X.39.4.341
Keaten, J. (2025, November 7). Denmark plans to ban access to social media for children under 15 | AP News. AP News. https://apnews.com/article/denmark-social-media-ban-children-7862d2a8cc590b4969c8931a01adc7f4
Keaten, J., & Press, T. A. (2025, November 7). Denmark to ban social media for anyone under 15 years old. Fortune. https://fortune.com/2025/11/07/denmark-social-media-ban-children-under-15/
Keşşafoğlu, D., Yıldız, E., Küntay, A., & A. Uzundağ, B. (2025). Infants’ background television exposure and maternal language input: A home observation study. Journal of Child Language, 1–17. https://doi.org/10.1017/S0305000925100391
Koob, G. F. (2013). Negative reinforcement in drug addiction: The darkness within. Current Opinion in Neurobiology, 23(4), 559–563. https://doi.org/10.1016/j.conb.2013.03.011
Koob, G. F., & Volkow, N. D. (2016). Neurobiology of addiction: A neurocircuitry analysis. The Lancet Psychiatry, 3(8), 760–773. https://doi.org/10.1016/S2215-0366(16)00104-8
Kuhl, P. K., Tsao, F.-M., & Liu, H.-M. (2003). Foreign-language experience in infancy: Effects of short-term exposure and social interaction on phonetic learning. Proceedings of the National Academy of Sciences, 100(15), 9096–9101. https://doi.org/10.1073/pnas.1532872100
Kuş, M. (2025). A meta-analysis of the impact of technology related factors on students’ academic performance. Frontiers in Psychology, 16, 1524645. https://doi.org/10.3389/fpsyg.2025.1524645
Law, E. C., Han, M. X., Lai, Z., Lim, S., Ong, Z. Y., Ng, V., Gabard-Durnam, L. J., Wilkinson, C. L., Levin, A. R., Rifkin-Graboi, A., Daniel, L. M., Gluckman, P. D., Chong, Y. S., Meaney, M. J., & Nelson, C. A. (2023a). Associations Between Infant Screen Use, Electroencephalography Markers, and Cognitive Outcomes. JAMA Pediatrics, 177(3), 311–318. https://doi.org/10.1001/jamapediatrics.2022.5674
Law, E. C., Han, M. X., Lai, Z., Lim, S., Ong, Z. Y., Ng, V., Gabard-Durnam, L. J., Wilkinson, C. L., Levin, A. R., Rifkin-Graboi, A., Daniel, L. M., Gluckman, P. D., Chong, Y. S., Meaney, M. J., & Nelson, C. A. (2023b). Associations Between Infant Screen Use, Electroencephalography Markers, and Cognitive Outcomes. JAMA Pediatrics, 177(3), 311–318. https://doi.org/10.1001/jamapediatrics.2022.5674
Library of Congress. (2025, January 14). Brazil: New Law Prohibits Cell Phone Use in Schools | Library of Congress. https://www.loc.gov/item/global-legal-monitor/2025-02-13/brazil-new-law-prohibits-cell-phone-use-in-schools/
Lichand, G., Moreno-Louzada, L., da Costa, T., & Gentzkow, M. (2026). The Educational Impacts of School Phone Bans: Evidence from Brazil.
Lillard, A. S., & Peterson, J. (2011). The Immediate Impact of Different Types of Television on Young Children’s Executive Function. Pediatrics, 128(4), 644–649. https://doi.org/10.1542/peds.2010-1919
Locker, P. (2024a, July 31). Cell Phone Ban in Russian Schools. Phone Locker. https://phonelocker.com/russian-school-cell-phone-ban/
Locker, P. (2024b, August 14). Dutch Schools Mobile Phone Ban. Phone Locker. https://phonelocker.com/dutch-schools-mobile-phone-ban/
Locker, P. (2024c, December 10). Norwegian Schools Phone Restrictions. Phone Locker. https://phonelocker.com/norwegian-schools-phone-restrictions/
Mallawaarachchi, S., Burley, J., Mavilidi, M., Howard, S. J., Straker, L., Kervin, L., Staton, S., Hayes, N., Machell, A., Torjinski, M., Brady, B., Thomas, G., Horwood, S., White, S. L. J., Zabatiero, J., Rivera, C., & Cliff, D. (2024). Early Childhood Screen Use Contexts and Cognitive and Psychosocial Outcomes: A Systematic Review and Meta-analysis. JAMA Pediatrics, 178(10), 1017–1026. https://doi.org/10.1001/jamapediatrics.2024.2620
Manolova, V., Pashina, I., Mateev, M., & Vezenkov, S. (2025). Munchausen Syndrome by Proxy and Other Forms of Parental Abuse in Children with Screen Addiction and a Diagnosis of Autism (ASD) and/or ADHD. Nootism, 1(2), 11–30. https://doi.org/10.64441/nootism.1.2.2
Manolova, V., & Vezenkov, S. (2025a). A qEEG-Derived Screen Reactivity Index Quantifies Pre–Post Changes After a 40-Day Digital Detox Despite Persistent Screen Addiction: Single-Case Evidence With Concurrent HRV. Nootism, 1(6), 13–30. https://doi.org/10.64441/nootism.1.6.2
Manolova, V., & Vezenkov, S. (2025b). Are Screen-Induced Synesthesia and Screen-induced Cue-Dependent Behavior Contributing Factors in the Misdiagnosis of ASD Among Children with Screen Addiction? Nootism, 1, 11–16. https://doi.org/10.64441/nootism.1.3.2
Manolova, V., & Vezenkov, S. (2025c). Parental Models: A Profile of the Dynamics in Children Dropping Out of Therapy Programs for Screen Addiction. Nootism, 1(1), 96–100. https://doi.org/10.64441/nootism.2NCSC.11
Manolova, V., & Vezenkov, S. (2025d). Screen Trauma – Specifics of the Disorder and Therapy in Adults and Children. Nootism, 1(1), 37–51. https://doi.org/10.64441/nootism.2NCSC.3
Manolova, V., & Vezenkov, S. (2025e). Screen-Mediated Developmental Deviation: A Historical-Cultural Theory of Autism’s Recognition and Rising Prevalence. Nootism, 1(6), 31–43. https://doi.org/10.64441/nootism.1.6.3
Manolova, V., & Vezenkov, S. (2025f). Unified Trauma-Addiction Functioning Model. Nootism, 1(4), 4–24. https://doi.org/10.64441/nootism.1.4.1
Mateev, M., Manolova, V., & Vezenkov, S. (2025). From Nonverbal to Language – How to Counteract Anti-Human Programming Controlling Children with Early Screen Addiction. Nootism, 1(1), 52–58. https://doi.org/10.64441/nootism.2NCSC.4
McArthur, B. A., Volkova, V., Tomopoulos, S., & Madigan, S. (2022). Global Prevalence of Meeting Screen Time Guidelines Among Children 5 Years and Younger: A Systematic Review and Meta-analysis. JAMA Pediatrics, 176(4), 373–383. https://doi.org/10.1001/jamapediatrics.2021.6386
McDaniel, B. T., & Radesky, J. S. (2018). Technoference: Parent Distraction With Technology and Associations With Child Behavior Problems. Child Development, 89(1), 100–109. https://doi.org/10.1111/cdev.12822
McDaniel, B. T., Ventura, A. K., Coyne, S. M., Wolfers, L. N., Pfafman, R., Shinde, A. S., Uva, S., Coleman, B., Ceja Almontes, K. I., & Galovan, A. M. (2026). Crying, Cradles, and Cellphones: A Longitudinal Examination of Infant Media Emotion Regulation and Socio-Emotional Development in Early Infancy. Infancy, 31(1), e70069. https://doi.org/10.1111/infa.70069
MCMC. (2025). Online Safety Act 2025 [Act 866] | Malaysian Communications And Multimedia Commission (MCMC). Malaysian Communications And Multimedia Commission (MCMC) | Suruhanjaya Komunikasi Dan Multimedia Malaysia (SKMM). https://www.mcmc.gov.my/en/legal/acts/communications-and-multimedia-amendment-act-20-1
Mineshita, Y., Kim, H.-K., Chijiki, H., Nanba, T., Shinto, T., Furuhashi, S., Oneda, S., Kuwahara, M., Suwama, A., & Shibata, S. (2021). Screen time duration and timing: Effects on obesity, physical activity, dry eyes, and learning ability in elementary school children. BMC Public Health, 21(1), 422. https://doi.org/10.1186/s12889-021-10484-7
Ministère du Travail, de la Santé, des Solidarités et des Familles. (2025, July 2). Protection de la petite enfance: Publication de l’arrêté interdisant l’exposition des enfants de moins de 3 ans aux écrans dans les lieux d’accueil du jeune enfant | solidarites.gouv.fr | Ministère du Travail et des Solidarités. https://solidarites.gouv.fr/protection-de-la-petite-enfance-publication-de-larrete-interdisant-lexposition-des-enfants-de-moins-de-3-ans-aux-ecrans-dans-les-lieux-daccueil-du-jeune-enfant
Morin, V. (2025, September 16). Pourquoi le dispositif « Portable en pause », pour que les élèves déposent leur téléphone dans des casiers, a été ignoré par la plupart des collèges. Le Monde. https://www.lemonde.fr/societe/article/2025/09/16/le-dispositif-portable-en-pause-boude-par-les-colleges-en-depit-des-annonces-de-rentree_6641345_3224.html
Mustonen, R., Torppa, R., & Stolt, S. (2022). Screen Time of Preschool-Aged Children and Their Mothers, and Children’s Language Development. Children, 9(10), 1577. https://doi.org/10.3390/children9101577
NAEP. (2022). NAEP Long-Term Trend Assessment Results: Reading and Mathematics. https://www.nationsreportcard.gov/highlights/ltt/2022/
NAEP. (2025, September 9). Nation’s Report Card Shows Declines in 8th-Grade Science and 12th-Grade Math and Reading; Last in a Series of Post-Pandemic NAEP Data. https://www.nagb.gov/news-and-events/news-releases/2025/declines-in-8th-grade-science-and-12th-grade-math-and-reading.html
Nishioka, T., Hasunuma, H., Okuda, M., Taniguchi, N., Fujino, T., Shimomura, H., Tanaka, Y., Shima, M., & Takeshima, Y. (2022). Effects of Screen Viewing Time on Sleep Duration and Bedtime in Children Aged 1 and 3 Years: Japan Environment and Children’s Study. International Journal of Environmental Research and Public Health, 19(7), 3914. https://doi.org/10.3390/ijerph19073914
NJDOE. (2026). New Jersey Department of Education Releases Updated Guidance on Bell to-Bell Policies to Prohibit Student Use of Cell Phones in Schools.
Nustad, S. H., & Abrahamsson, L. M. (2026). Passive and active screen time relate differently to attention in preschool children. Frontiers in Psychology, 17. https://doi.org/10.3389/fpsyg.2026.1737937
Ornitz, E. M. (1974). Effect of Visual Input on Vestibular Nystagmus in Autistic Children. Archives of General Psychiatry, 31(3), 369. https://doi.org/10.1001/archpsyc.1974.01760150075011
Ortiz De Gortari, A. B., & Gackenbach, J. (2021). Game Transfer Phenomena and Problematic Interactive Media Use: Dispositional and Media Habit Factors. Frontiers in Psychology, 12, 585547. https://doi.org/10.3389/fpsyg.2021.585547
Ortiz de Gortari, A. B., & Griffiths, M. D. (2014). Automatic Mental Processes, Automatic Actions and Behaviours in Game Transfer Phenomena: An Empirical Self-Report Study Using Online Forum Data. International Journal of Mental Health and Addiction, 12(4), 432–452. https://doi.org/10.1007/s11469-014-9476-3
Pashina, I., Manolova, V., & Vezenkov, S. (2025). Parental Recovery as a Key Factor for the Recovery of Children with Screen Addiction – Biofeedback Therapy for Severe Disorders. Nootism, 1(1), 83–89. https://doi.org/10.64441/nootism.2NCSC.9
Pempek, T. A., Kirkorian, H. L., & Anderson, D. R. (2014). The Effects of Background Television on the Quantity and Quality of Child-Directed Speech by Parents. Journal of Children and Media, 8(3), 211–222. https://doi.org/10.1080/17482798.2014.920715
Pessoa, G. (2025, February 6). New law in Brazil is making students put away their smartphones at school. AP News. https://apnews.com/article/brazil-bill-phones-schools-restrictions-20b95516d6e2a0f63ebb642defba964b
Petrov, P., Dimova, V., Manolova, V., & Vezenkov, S. (2025). Screen Time and Policy Approaches to Digital Media Use in Nurseries, Kindergartens, and Schools Worldwide: A Critical Analysis. Nootism, 1(2), 41–50. https://doi.org/10.64441/nootism.1.2.4
Petrov, P., Manolova, V., & Vezenkov, S. (2025). Hidden Family Dynamics in a Case Study of a Child with Screen Addiction, Hyperactivity, and Language Deficits. Nootism, 1(1), 90–95. https://doi.org/10.64441/nootism.2NCSC.10
Petrova, S., Manolova, V., & Vezenkov, S. (2025). Reintroducing Screens: Severe Regression and Symptom Aggravation in Children with ASD/Screen Addiction. Nootism, 1(1), 59–65. https://doi.org/10.64441/nootism.2NCSC.5
PIRG, U. (2025, November 13). Trouble in Toyland 2025: A.I. bots and toxics present hidden dangers. U.S. PIRG Education Fund. https://pirg.org/edfund/resources/trouble-in-toyland-2025-a-i-bots-and-toxics-represent-hidden-dangers/
Porges, S. W. (2007). The polyvagal perspective. Biological Psychology, 74(2), 116–143. https://doi.org/10.1016/j.biopsycho.2006.06.009
Porges, S. W. (2021). Polyvagal Theory: A biobehavioral journey to sociality. Comprehensive Psychoneuroendocrinology, 7, 100069. https://doi.org/10.1016/j.cpnec.2021.100069
Porges, S. W. (2025). Deconstructing Autism Through the Lens of the Polyvagal Theory: A foreword to Understanding Autism edited by Drs. Papaneophytou and Das. In Understanding Autism (pp. xxiii–xxx). Elsevier. https://doi.org/10.1016/B978-0-443-27366-7.09998-3
Pugh. (2026, February 2). Where are smartphones banned in primary schools in Germany? The Local Germany. https://www.thelocal.de/20260202/where-are-smartphones-banned-in-primary-schools-in-germany
RADAM, M., BILLONES, J., MASCARIÑA, E., LEBAS, T., & Decena III, J. (2026). SMARTPHONE ADDICTION AND ACADEMIC PERFORMANCE AMONG ACCOUNTANCY, BUSINESS AND MANAGEMENT STUDENTS AT TACURONG NATIONAL HIGH SCHOOL. https://doi.org/10.13140/RG.2.2.17395.90408
Reuters. (2026, March 18). Poland plans to ban mobile phone use by under-16s in schools. Reuters. https://www.reuters.com/business/media-telecom/poland-plans-ban-mobile-phone-use-by-under-16s-schools-2026-03-18/
Reynolds, M., Esfandiari, M., & O’Higgins Norman, J. (2025, January 8). Restriction or Resilience? Smartphone Bans in Schools: A Qualitative Study on the Experiences of Students and Teachers. https://www.dcu.ie/antibullyingcentre/restriction-or-resilience
Rizzolatti, G., & Craighero, L. (2004). THE MIRROR-NEURON SYSTEM. Annual Review of Neuroscience, 27(Volume 27, 2004), 169–192. https://doi.org/10.1146/annurev.neuro.27.070203.144230
Rizzolatti, G., & Sinigaglia, C. (2016). The mirror mechanism: A basic principle of brain function. Nature Reviews. Neuroscience, 17(12), 757–765. https://doi.org/10.1038/nrn.2016.135
RTL Today, object. (2025, April 4). 22 April & 2 June: Luxembourg schools to enforce staged smartphone bans. RTL today. RTL Today. https://today.rtl.lu/news/luxembourg/luxembourg-schools-to-enforce-staged-smartphone-bans-2291437
Saeima Press Service. (2024, November 10). Children up to grade 6 banned from using mobile phones in schools. Saeima.Lv. https://www.saeima.lv/en/news/saeima-news/33941-children-up-to-grade-6-banned-from-using-mobile-phones-in-schools
Sanders, T., Parker, P. D., Del Pozo-Cruz, B., Noetel, M., & Lonsdale, C. (2019). Type of screen time moderates effects on outcomes in 4013 children: Evidence from the Longitudinal Study of Australian Children. The International Journal of Behavioral Nutrition and Physical Activity, 16(1), 117. https://doi.org/10.1186/s12966-019-0881-7
Sevinc, N. T. (2025, June 16). Italy bans cellphone use in high schools during education hours. Anadolu. https://www.aa.com.tr/en/europe/italy-bans-cellphone-use-in-high-schools-during-education-hours/3600936
Sharma, A. (2026, May 8). 1 year post cellphone ban in Quebec schools, here's how these students are adjusting. CBC News. https://www.cbc.ca/news/canada/montreal/cell-phone-ban-quebec-schools-students-9.7189776
Stefanova, M., Manolova, V., & Vezenkov, S. (2025). ADHD and Screen Addiction in Children Aged 3-9: Staged Recovery and Neurophysiological Markers. Nootism, 1(1), 66–73. https://doi.org/10.64441/nootism.2NCSC.6
Strouse, G. A., & Samson, J. E. (2021). Learning From Video: A Meta-Analysis of the Video Deficit in Children Ages 0 to 6 Years. Child Development, 92(1), e20–e38. https://doi.org/10.1111/cdev.13429
Sundqvist, A., Barr, R., Heimann, M., Birberg-Thornberg, U., & Koch, F.-S. (2024). A longitudinal study of the relationship between children’s exposure to screen media and vocabulary development. Acta Paediatrica, 113(3), 517–522. https://doi.org/10.1111/apa.17047
Swingle, M. K. (2019). i-Minds - 2nd edition: How and Why Constant Connectivity is Rewiring Our Brains and What to Do About it. New Society Publishers.
Swingle, M. K., & Swingle, P. G. (2016). Are You Sure It’s AD(H)D? Biofeedback, 44(1), 35–41. https://doi.org/10.5298/1081-5937-44.1.05
Swingle, P. G. (2002). Parameters Associated with Rapid Neurotherapeutic Treatment of Common ADD (CADD). Journal of Neurotherapy, 5(4), 73–84. https://doi.org/10.1300/J184v05n04_05
Today, H. (2024, September 2). Ban on Mobile Phones in Schools Takes Effect from Today. Hungary Today. https://hungarytoday.hu/ban-on-mobile-phones-in-schools-takes-effect-from-today/
Tomopoulos, S., Dreyer, B. P., Berkule, S., Fierman, A. H., Brockmeyer, C., & Mendelsohn, A. L. (2010). Infant media exposure and toddler development. Archives of Pediatrics & Adolescent Medicine, 164(12), 1105–1111.
Tronick, E. (2007). The neurobehavioral and social-emotional development of infants and children (pp. xii, 571). W. W. Norton & Company.
- (2025, December 10). Social media: Age-related bans won’t keep kids safe, UNICEF warns | UN News. https://news.un.org/en/story/2025/12/1166557
UNESCO. (2026, May 10). Phone bans in schools are spreading worldwide as the policy debate rages on | Global Education Monitoring Report. https://www.unesco.org/gem-report/en/articles/phone-bans-schools-are-spreading-worldwide-policy-debate-rages
Uzundağ, B. A., Altundal, M. N., & Keşşafoğlu, D. (2022). Screen Media Exposure in Early Childhood and Its Relation to Children’s Self-Regulation. Human Behavior and Emerging Technologies, 2022, 1–34. https://doi.org/10.1155/2022/4490166
Uzundağ, B. A., Güven, İ. N., Sıvış, Ö., & Başpınar, G. (2026). Screen Media Exposure and Inhibitory Control: A Longitudinal Study From Infancy to Toddlerhood. Infancy: The Official Journal of the International Society on Infant Studies, 31(1), e70067. https://doi.org/10.1111/infa.70067
Ventura, A. K., & Teitelbaum, S. (2017). Maternal distraction during breast-and bottle feeding among WIC and non-WIC mothers. Journal of Nutrition Education and Behavior, 49(7), S169–S176.
Veraksa, N., Veraksa, A., Gavrilova, M., Bukhalenkova, D., Oshchepkova, E., & Chursina, A. (2021). Short- and Long-Term Effects of Passive and Active Screen Time on Young Children’s Phonological Memory. Frontiers in Education, 6. https://doi.org/10.3389/feduc.2021.600687
Vezenkov, S., & Manolova, V. (2025a). Gaming and Gambling Addiction in Fathers as a Risk Factor for Early Screen Addiction in Children. Nootism, 1(2), 31–40. https://doi.org/10.64441/nootism.1.2.3
Vezenkov, S., & Manolova, V. (2025b). Neurobiology of Autism/Early Screen Addiction Recovery. Nootism, 1, 19–36. https://doi.org/10.64441/nootism.2NCSC.2
Vezenkov, S., & Manolova, V. (2025c). Screen Addiction – Biomarkers, Developmental Damage and Recovery. Nootism, 1(1), 6–18. https://doi.org/10.64441/nootism.2NCSC.1
Vezenkov, S., & Manolova, V. (2025d). Screen-Induced Pathological Eye-Covering Reflex in Children with Early Screen Addiction. Nootism, 1(3), 5–10. https://doi.org/10.64441/nootism.1.3.1
Vezenkov, S., & Manolova, V. (2025e). Screen-Induced Pathological Vestibular Reflex: A Specific Marker of Early Screen Addiction. Nootism, 1(2), 5–10. https://doi.org/10.64441/nootism.1.2.1
Vezenkov, S., & Manolova, V. (2025f). Sensory Disintegration versus Sensory Deprivation: Vestibular-Visual Dynamics and Shared Behavioral Phenotypes in ASD and Early Blindness. Nootism, 1(6), 4–12. https://doi.org/10.64441/nootism.1.6.1
Vezenkov, S., & Manolova, V. (2026). Screen Addiction in Children and Adults: Biomarkers, Screen Trauma and Reversed Development. Nootism, 2(1), 4–45. https://doi.org/10.64441/nootism.2.1.1
Volkow, N. D., Michaelides, M., & Baler, R. (2019). The Neuroscience of Drug Reward and Addiction. Physiological Reviews, 99(4), 2115–2140. https://doi.org/10.1152/physrev.00014.2018
Wilkinson, C. L., Yankowitz, L. D., Chao, J. Y., Gutiérrez, R., Rhoades, J. L., Shinnar, S., Purdon, P. L., & Nelson, C. A. (2024). Developmental trajectories of EEG aperiodic and periodic components in children 2–44 months of age. Nature Communications, 15(1), 5788. https://doi.org/10.1038/s41467-024-50204-4
Wilkinson, O. M. | I. (2025, March 20). Austria to ban phones in schools. https://www.thetimes.com/world/europe/article/austria-smartphone-ban-schools-concentration-3nnwqwj5h
Wilks, A. (2026, April 23). Turkish parliament passes bill to restrict social media access for under-15s. AP News. https://apnews.com/article/turkey-social-media-children-restrictions-law-d88963a7446a12cf4963b73d455b5ef7
Zablotsky, B., Arockiaraj, B., Haile, G., & Ng, A. (2024, October 29). Daily Screen Time Among Teenagers: United States, July 2021–December 2023—Data Briefs—Number 513 -October 2024. Centers for Disease Control and Prevention. https://doi.org/10.15620/cdc/168509
Zhao, Y., Han, X., Bagot, K. S., Tapert, S. F., Potenza, M. N., & Paulus, M. P. (2025). Examining measurement discrepancies in adolescent screen media activity with insights from the ABCD study. Npj Mental Health Research, 4(1), 15. https://doi.org/10.1038/s44184-025-00131-z
Zivan, M., Bar, S., Jing, X., Hutton, J., Farah, R., & Horowitz-Kraus, T. (2019). Screen-exposure and altered brain activation related to attention in preschool children: An EEG study. Trends in Neuroscience and Education, 17, 100117. https://doi.org/10.1016/j.tine.2019.100117