

Stoyan R. Vezenkov
Center for applied neuroscience Vezenkov, BG-1582 Sofia, e-mail: info@vezenkov.com
For citation: Vezenkov S.R. (2026) The Missing Defensive State in Wearable and HRV-Based Stress Algorithms. A Trauma–Informed Critique of Polar and Kubios Interpretations. Nootism 2(2), 4-16, https://doi.org/10.64441/nootism.2.2.1
Abstract
Consumer wearables and heart rate variability (HRV) analysis platforms increasingly provide stress, recovery, readiness, parasympathetic, sympathetic, and autonomic balance scores derived from heart rate, HRV, respiration, sleep, and movement. These tools are valuable because they provide ecologically valid physiological data outside the laboratory. However, their clinical interpretation becomes problematic in trauma-informed practice. Clinically observed low-arousal defensive states may present with low heart rate, low movement, reduced or rigid HRV, flattened respiratory – linked variability, dissociation, and collapse-like behavior. Such patterns may not represent restorative calm. They may instead represent low-arousal defensive immobilization – a state often described in polyvagal terms as dorsal-vagal-like shutdown, although the precise neurophysiological substrate remains debated.
This paper argues that current wearable and HRV-based stress/recovery models often organize autonomic physiology along a simplified continuum: stress versus recovery, sympathetic activation versus parasympathetic restoration, or low versus high physiological load. Polar's Nightly Recharge estimates overnight recovery through heart rate, RMSSD– based HRV, and breathing rate during the early hours of sleep compared with a personal baseline. Kubios HRV, a professional scientific platform, calculates parasympathetic and sympathetic indices using mean NN interval, RMSSD, SD1, mean heart rate, Baevsky's Stress Index, and SD2. These models are useful for many recovery and activation contexts, but their public output categories do not adequately represent low– arousal defensive immobilization and may therefore conflate bradycardic hypoarousal with recovery or with ambiguous stress/recovery states.
The central claim is not that these systems measure incorrectly, but that their interpretive categories are incomplete. A low heart rate, low HRV, low movement state may be scored or understood as low stress, recovery, or ambiguous autonomic strain, while clinically it may correspond to freeze, shutdown, dissociative hypoarousal, or autonomic rigidity. This claim does not require the validity of contested anatomical postulates of polyvagal theory, recently challenged in an international expert evaluation (Grossman, 2023; Grossman et al., 2026); it requires only the recognition that defensive immobilization with cardiac deceleration is a well-documented psychophysiological phenomenon (Roelofs, 2017). A worked geometric analysis of the NN-interval distribution illustrates how Baevsky's Stress Index – the basis of the Kubios Stress Index and one component of the Kubios SNS Index – can produce paradoxically elevated values in bradycardic low-arousal states despite simultaneous low heart rate. This paper proposes a three-state interpretive framework distinguishing restorative regulation, sympathetic mobilization, and low-arousal defensive immobilization, and proposes preliminary criteria for a Low Arousal Defensive State Index (LADSI) to guide future research and trauma-informed clinical interpretation.
Keywords: heart rate variability (HRV), Polar, Kubios, RMSSD, respiratory sinus arrhythmia (RSA), Baevsky stress index, trauma, dissociation, freezing, low arousal defensive immobilization, polyvagal theory, wearable devices, autonomic state ontology
- Introduction: The Clinical Problem
Consumer wearables and HRV platforms are increasingly used not only in sport and wellness but also in psychotherapy, trauma therapy, rehabilitation, and self-monitoring. Patients bring data from Polar, Garmin, Oura, WHOOP, Apple Watch, Kubios, and other devices into clinical conversations as evidence of stress, recovery, readiness, sleep quality, and autonomic functioning. This creates an opportunity: clinicians gain access to real– world physiological data across days and nights. It also creates a risk: device– derived scores may be interpreted as if they directly represent psychological safety, emotional distress, trauma activation, or nervous system state.
This risk is particularly important in trauma– informed practice. Many trauma patients do not present only with hyperarousal. They may also present with hypoarousal, collapse, emotional numbness, dissociation, immobilization, and shutdown– like states. These states may be accompanied by low movement and low heart rate, which can easily be confused with calmness, rest, or recovery if interpreted through a simple stress–recovery model. A recent living umbrella review of consumer wearable technologies concluded that such devices are widely used in clinical and non-clinical populations, while the accuracy of biometric outcomes such as heart rate, sleep, and physical activity varies across devices and contexts (Doherty et al., 2024). A separate evaluation of fourteen composite health scores from ten leading wearable manufacturers found that the underlying formulas are typically not disclosed and that peer-reviewed evidence for these composite scores remains limited (Doherty et al., 2025).
The problem addressed here is not primarily sensor accuracy. It is state interpretation. A sensor may correctly detect low heart rate, low RMSSD, low respiratory-linked variability, or low movement. The clinical question is different: What does that physiological configuration mean in this person, in this context, at this moment?
The argument proceeds as follows. Sections 2 and 3 examine two paradigmatic algorithms – Polar's Nightly Recharge in the consumer domain and Kubios's PNS, SNS, and Stress indices in the research domain – and identify the limits of their interpretive categories. Section 4 reviews the broader case for caution in inferring autonomic state from HRV alone. Section 5 takes a deliberately conservative position on polyvagal theory, recognizing the recent international expert critique while preserving the core clinical insight. Section 6 reviews the freezing and defensive bradycardia literature as an independent foundation for the central claim. Sections 7 and 8 develop the formal argument and present a worked geometric example of how the Baevsky– based stress index in Kubios can produce paradoxical outputs in low– arousal defensive states. Section 9 proposes a three-state interpretive framework. Section 10 introduces a preliminary research construct, the Low– Arousal Defensive State Index (LADSI). Sections 11–14 address clinical implications, implications for the peer-reviewed literature, a research agenda, and limitations.
A note on terminology. Throughout this paper, NN interval denotes the normal to normal interbeat interval. BR or breathing rate denotes respiration rate; we deliberately avoid the abbreviation RR because of potential confusion between R–R intervals and respiratory rate. Low-arousal defensive immobilization is used as the primary clinical physiological term; dorsal–vagal–like shutdown is used as a secondary, polyvagal framework descriptor where appropriate.
- Polar: A Recovery Algorithm, Not a Trauma– State Classifier
Polar's Nightly Recharge is a sophisticated overnight recovery model. It combines Sleep Charge and ANS Charge to estimate how well the body has recovered from recent stressors such as training, work, lifestyle load, and other demands. The ANS Charge component is based on heart rate, HRV (computed as RMSSD), and breathing rate during a four– hour period beginning approximately thirty minutes after sleep onset. These values are compared with the user's usual levels calculated from the previous twenty eight days. Polar states that the greatest weight is given to heart rate and the least to breathing rate, while RMSSD is the selected HRV parameter reflecting parasympathetic activation (Polar, n.d., Nightly Recharge White Paper).
This is appropriate for a recovery algorithm. Nighttime is a relatively controlled measurement context: posture, activity level, environment, and time of day are more stable than during daytime. Polar explicitly frames Nightly Recharge as a way to assess overnight recovery, and the early hours of sleep are selected because they may be more sensitive to recovery from work and exercise than whole– night averages.
However, this design also defines the limit of interpretation. The Polar model asks something like:
- Did the autonomic system settle during early sleep compared with this person's usual pattern?
It does “not” ask:
- Is this person in a state of safety, dissociation, freeze, collapse, or trauma– related shutdown?
A Polar– like model may correctly identify that heart rate is low or that the body is inactive. But in a trauma patient, low heart rate and low movement are not sufficient evidence of safety. They may also be part of low– arousal defensive immobilization.
The problem becomes sharper when HRV is also low. In a simple recovery model, lower heart rate pulls interpretation toward recovery, while lower RMSSD pulls interpretation toward poorer recovery or higher autonomic strain. The result may be a mixed or compromised score. But the clinical meaning may be neither ordinary recovery nor ordinary sympathetic stress. It may be a third state: low-arousal defense.
It must be acknowledged that Polar's documentation explicitly disclaims that "HRV measures do not identify the specific source of stress" (Polar, n.d.). That disclaimer is honest but understates the problem. The issue is not only that the algorithm cannot identify what causes low HRV; it is that the algorithm's output categories – recovery and lack of recovery – do not contain a representation of defensive immobilization at all.
- Kubios: Strong HRV Analysis, Incomplete State Ontology
Kubios HRV is not a consumer toy. It is a serious HRV analysis platform used widely in research and professional settings. Its strengths include preprocessing, artifact correction, time– domain analysis, frequency-domain analysis, nonlinear analysis, and time-varying HRV analysis. The critique here is therefore not that Kubios fails as HRV software. The critique is that even advanced HRV interpretation can remain trapped in a two branch autonomic ontology when applied clinically to trauma states.
Kubios describes its “PNS Index” as a composite calculated from mean NN interval, RMSSD, and normalized Poincaré SD1. It describes its “SNS Index” as a composite calculated from mean heart rate, Baevsky's Stress Index, and normalized Poincaré SD2. Kubios states that the PNS Index reflects recovery and relaxation states, typically associated with lower heart rate and higher HRV, whereas the SNS Index reflects stress responses, typically associated with higher heart rate and lower HRV. The exact weighting is proprietary (Kubios, 2024).
It is important to note that the SNS Index is “not” equivalent to Baevsky's Stress Index alone. Mean HR and Baevsky SI are weighted alongside SD2 in the composite. This means that, in a bradycardic low– arousal state, mean HR pulls the SNS Index downward (toward lower sympathetic) while Baevsky SI may pull it upward (toward higher sympathetic). The composite SNS Index therefore becomes ambiguous in such states rather than uniformly elevated. This nuance, while important, does not weaken the central argument; it relocates it. The problem is not that Kubios will declare a defensive immobilization patient "stressed." The problem is that Kubios's two– axis output (PNS recovery vs. SNS stress) has no category that meaningfully captures the state.
Kubios also calculates a “Stress Index” based on Baevsky's Stress Index. Baevsky's index is a geometric measure derived from the NN-interval histogram:
where “AMo” is the mode amplitude, expressed as a percentage value (e.g., 25 for 25%, not 0.25 as a proportion); “Mo” is the modal NN interval (most frequent value, in seconds); and “MxDMn” is the variation scope (the difference between the longest and shortest NN intervals, in seconds). If AMo is expressed as a proportion rather than a percentage, the numerator becomes 100 × AMo. Kubios applies detrending to remove very low frequency components and reports the square root of the original Baevsky SI to make the distribution closer to normal (Baevsky & Chernikova, 2017; Kubios, 2024).
The historical context of this index is important. Baevsky's Stress Index was developed in the context of Soviet space medicine in the 1960s for assessing acute autonomic strain in cosmonauts (Parin et al., 1965) (Baevsky & Chernikova, 2017). Its target physiological state was acute sympathetic mobilization. It was not designed, and has not been formally validated, for distinguishing chronic immobilization states from rest in clinical populations.
This is physiologically important. The Baevsky/Kubios Stress Index is sensitive to narrowing and modal concentration of the NN-interval distribution. It may correctly detect reduced variability or rhythm rigidity. But the label stress should not be equated automatically with sympathetic fight or flight activation. A narrow NN distribution can arise from sympathetic mobilization, but it can also arise from autonomic rigidity, fatigue, medication effects, illness, respiratory suppression, sleep-stage effects, or trauma-related hypoarousal. We will return to this point with a worked geometric analysis in Section 8.
Kubios therefore may detect an abnormal or rigid cardiovascular pattern, yet its public output categories do not determine whether the state is restorative, mobilized, or defensively immobilized. This is the deeper structural limit.
- Why HRV and RSA Cannot Carry the Full Clinical Meaning
HRV is a valuable non– invasive measure of cardiac autonomic regulation, but it is not a direct measurement of psychological stress, subjective safety, central vagal drive, or trauma state. The Task Force standards for HRV measurement emphasized that HRV interpretation requires attention to recording duration, physiological context, and methodological detail (Task Force, 1996).
RMSSD and SD1 are commonly interpreted as reflecting cardiac parasympathetic modulation. However, this interpretation becomes unstable when respiration, posture, activity, sleep stage, medication, illness, or emotional context changes. RSA in particular is vulnerable to overinterpretation. Grossman and Taylor (2007) argued that RSA or high– frequency HRV is often used as an index of cardiac vagal tone, but respiratory parameters, physical activity, beta– adrenergic tone, and other factors confound the relation between RSA and vagal tone; RSA and cardiac vagal tone can dissociate under some circumstances (Grossman & Taylor, 2007).
The same caution applies to sympathetic inference from HRV. Billman (2013) criticized the widespread use of LF/HF as a measure of sympathovagal balance, arguing that the metric rests on problematic assumptions: that LF power mainly reflects sympathetic activity, that HF power purely reflects parasympathetic activity, that sympathetic and parasympathetic activity change reciprocally, and that their interaction is linear (Billman, 2013; Boudreau et al., 2013). None of these assumptions holds robustly across physiological contexts.
The implication for trauma– informed interpretation is direct: low HRV is not one thing. It may represent sympathetic arousal, poor recovery, illness, overtraining, inflammation, respiratory change, medication, sleep disruption, autonomic rigidity, dissociative hypoarousal, or defensive immobilization. HRV can inform clinical reasoning, but it cannot replace clinical state assessment (Shaffer & Ginsberg, 2017).
- Polyvagal Theory: Useful Clinical Map, Contested Physiology
Polyvagal theory has been clinically influential because it distinguishes more than one defensive autonomic pattern. In Porges's formulation, autonomic regulation is organized hierarchically and includes a ventral vagal pathway supporting social engagement and physiological flexibility, the sympathetic nervous system supporting active mobilization, and a more primitive dorsal vagal pathway supporting immobilization and shutdown– like patterns. Porges's recent overview presents the theory as a framework for social engagement, emotional resilience, neuroception, co– regulation, and trauma-informed clinical practice (Porges, 2025).
However, polyvagal theory is scientifically contested. In a major recent expert evaluation, Grossman and 38 co-authoring specialists in vagal physiology and vertebrate evolution – many cited by polyvagal literature as supporting the theory – published a comprehensive critique arguing that several core neurophysiological and evolutionary claims of polyvagal theory are not defensible on the basis of existing evidence (Grossman et al., 2026). Their concerns include the proposed division of mammalian cardiac vagal control between nucleus ambiguus and dorsal motor nucleus of the vagus, the interpretation of RSA as a marker of distinct vagal pathways, and the evolutionary narrative of mammalian "repurposing" of vagal circuitry. Porges has responded in the same journal, arguing the critics evaluate a distorted version of the theory; the debate is active and ongoing.
For this reason, the argument in this paper is deliberately conservative. It does not require accepting every anatomical claim of polyvagal theory. It does not claim that Polar, Kubios, RMSSD, RSA, or Baevsky's Stress Index can directly measure ventral or dorsal vagal activity. They cannot.
The narrower and more defensible claim is this:
Trauma– informed wearable and HRV interpretation requires at least three functional autonomic categories: restorative regulation, sympathetic mobilization, and low– arousal defensive immobilization.
This claim is compatible with polyvagal clinical language, but it does not depend on polyvagal anatomy. Because the anatomical specificity of PVT remains contested, the present argument uses PVT primarily as a clinical state framework and does not infer dorsal vagal efferent activity directly from HRV. The framework can be grounded entirely in the well– established psychophysiology of freezing and defensive bradycardia, to which we now turn.
- Freezing and Defensive Bradycardia: Low Arousal Is Not Always Recovery
The argument does not depend solely on PVT. The broader defensive freezing literature supports the same clinical concern. Freezing is not restorative rest; it is a defensive state involving immobility, heightened threat processing, action preparation, and parasympathetically dominated heart rate deceleration. Roelofs (2017) describes freezing as attentive immobility associated with bradycardia – distinct from sympathetically dominated fight or flight – and emphasizes its relevance for human stress-coping and threat– processing in psychiatric populations (Roelofs, 2017).
Human studies often operationalize freezing through both heart rate deceleration and postural immobility. In approach–avoidance studies, freezing during threat anticipation has been measured using bradycardia together with body sway, confirming that heart rate deceleration can be part of a threat anticipatory freezing response rather than a sign of calm (Felitti et al., 1998; Hashemi et al., 2019; Niermann et al., 2017). This pattern has been observed not only in laboratory threat paradigms but also in clinical populations with anxiety, PTSD, and trauma exposure.
This distinction is clinically decisive. A wearable or HRV platform may interpret low heart rate and low movement as rest. But in a trauma patient, the same pattern may reflect immobilization under threat. The physiological signal is real; the meaning is underdetermined. HRV-based algorithms that do not model this distinction risk assigning the same physiological surface pattern to the wrong clinical state.
Trauma-related dissociation further complicates the picture. A systematic review of the autonomic correlates of trauma-related dissociation in PTSD samples found that neurophysiological models often link dissociation to hypoarousal or blunted autonomic response, but that empirical findings across physiological markers are inconsistent (Beutler et al., 2022). That inconsistency does not weaken the present argument – it strengthens it. If dissociation and shutdown do not have one universal HRV signature, then HRV only or HRV heavy algorithms cannot reliably classify them as a single category, and the algorithms' two-state output ontology cannot accommodate this heterogeneity at all.
The freezing literature thus provides an independent foundation: low– arousal defensive states with cardiac deceleration are well– documented psychophysiological phenomena. Whether one accepts polyvagal theory's specific anatomical account or not, the clinical and physiological reality of these states is not in dispute. The gap is in the interpretive categories of current algorithms.
- The Blind Spot: Two Signals, Three Meanings
The core problem can be summarized as follows.
|
Physiological pattern |
Common algorithmic interpretation |
Trauma– informed alternative |
|
Low HR + high HRV/RSA + stable breathing + subjective safety |
Recovery / low stress |
Restorative regulation |
|
High HR + low HRV/RSA + faster breathing + activation |
Stress / sympathetic load |
Mobilization (fight-flight) |
|
Low HR + low HRV/RSA + low movement + numbness/collapse/dissociation |
Ambiguous; sometimes low stress, poor recovery, or autonomic strain |
Low– arousal defensive immobilization |
The third pattern is the missing state.
For Polar, this blind spot appears because the model is designed to estimate recovery, especially during sleep. A low heart rate may support a better recovery interpretation, while low RMSSD may reduce ANS Charge. But the algorithm is not designed to determine whether a low-arousal state is restorative or defensive. (Boudreau et al., 2013)
For Kubios, the blind spot is subtler. Kubios may detect reduced variability through RMSSD, SD1, SD2, and Stress Index. But its PNS/SNS interpretive framework still maps signals onto a relaxation/recovery versus stress/sympathetic response axis. In a patient with low heart rate and low HRV, mean NN interval may pull the PNS Index upward, RMSSD and SD1 may pull it downward; mean HR may pull the SNS Index downward, while the Baevsky Stress Index may pull the SNS Index upward if NN intervals are narrow and modal. The result may be mathematically valid but clinically ambiguous – and the ambiguity is rarely flagged to the user.
The conceptual structure of this mismatch is illustrated in Figure 1. Panel A shows a PVT-inspired three–state clinical model – presented for clinical clarity, while explicitly noting that the model's anatomical specificity remains debated. Panel B shows the binary axis on which current algorithms operate, and the projection problem: while restorative regulation and sympathetic mobilization map onto the axis correctly, low-arousal defensive immobilization has no stable mapping. Its low–HR signal pulls the algorithmic output toward "recovery"; its low HRV signal (and corresponding elevated raw Baevsky SI) pulls toward "stress." A second, vertical axis – arousal level, ranging from mobilization/engagement to immobilization/collapse – is the missing dimension required to make these states distinguishable.
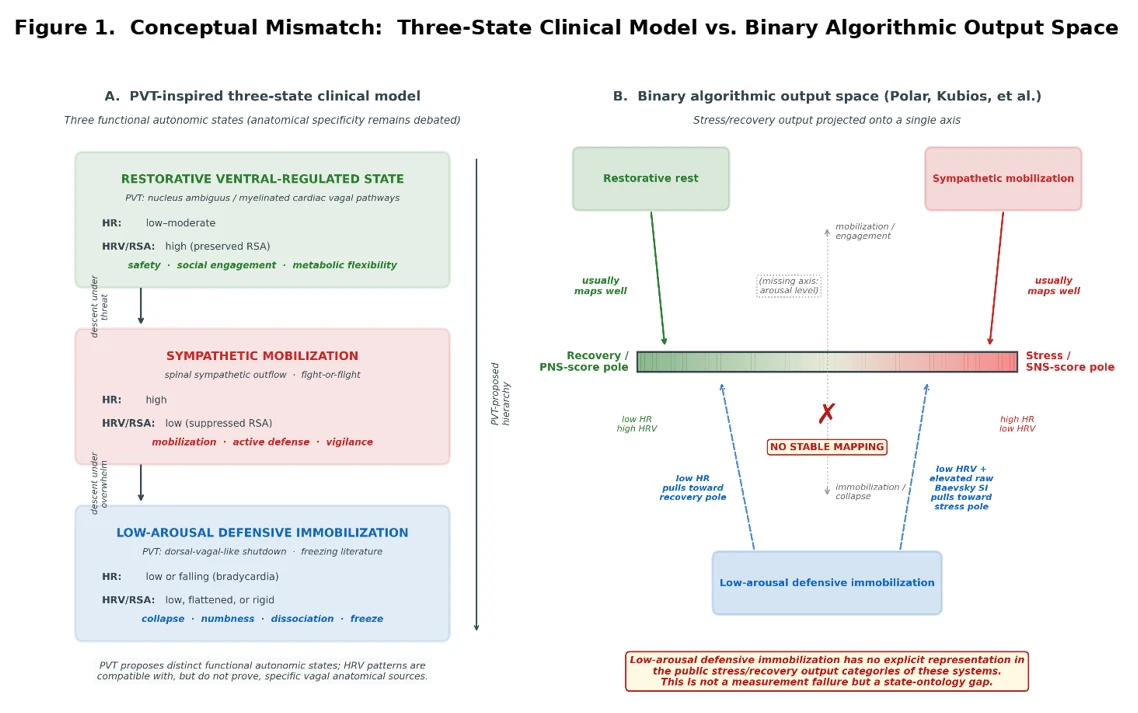
Figure 1. Conceptual mismatch between a three– state trauma– informed autonomic model and two– branch HRV stress/recovery outputs. Panel A shows a PVT– inspired clinical model in which autonomic states are organized functionally as restorative ventral– regulated rest, sympathetic mobilization, and low-arousal defensive immobilization. The anatomical mapping of these states remains debated; the figure is intended as a clinical state model, not as evidence that HRV directly identifies specific vagal nuclei. PVT proposes distinct functional autonomic states; HRV patterns are compatible with, but do not prove, specific vagal anatomical sources. Panel B shows the simplified output space of many HRV-based stress/recovery models, in which signals are projected onto a recovery/PNS score pole versus a stress/SNS score pole. Restorative rest and sympathetic mobilization usually map onto this axis in clinically intelligible ways. Low-arousal defensive immobilization does not: its bradycardia pulls interpretation toward recovery, while its low HRV, low RSA, and elevated raw Baevsky SI pull interpretation toward stress. The result is not measurement failure but state-ontology failure: the algorithm lacks a third category for bradycardic defensive immobilization. The dashed vertical "arousal level" axis represents the missing dimension that would be required to distinguish restorative from defensive low-arousal states.
The missing variable is not another HRV metric. The missing variable is a third state model.
- The Geometric Anatomy of Baevsky SI Non– Specificity: A Worked Example
The following simulations are not intended to diagnose dorsal vagal activity from HRV. Rather, they illustrate a mathematical and interpretive problem: two physiologically different states can produce similarly narrow NN-interval distributions and therefore elevated raw Baevsky SI. The physiological origin of that narrowing cannot be determined from SI alone.
8.1 Three reference profiles
Consider three 60 second cardiac recordings drawn from individuals in three distinct autonomic states:
- Profile A (Restorative ventral– regulated rest): mean HR 60 bpm, prominent respiratory-linked oscillation, broad NN– interval distribution, RMSSD ≈ 126 ms.
- Profile B (Sympathetic mobilization): mean HR 90 bpm, suppressed RSA, narrow NN-interval distribution centered at high HR, RMSSD ≈ 31 ms.
- Profile C (Low-arousal defensive immobilization, dorsal-vagal-like): mean HR 52 bpm (bradycardia), suppressed RSA, narrow NN-interval distribution centered at low HR, RMSSD ≈ 39 ms.
These profiles are visualized in Figure 2. The top row shows simulated heart– rate traces; the bottom row shows the corresponding NN-interval distributions with annotated Baevsky parameters and computed raw SI values, alongside their square root transformations as reported by Kubios.
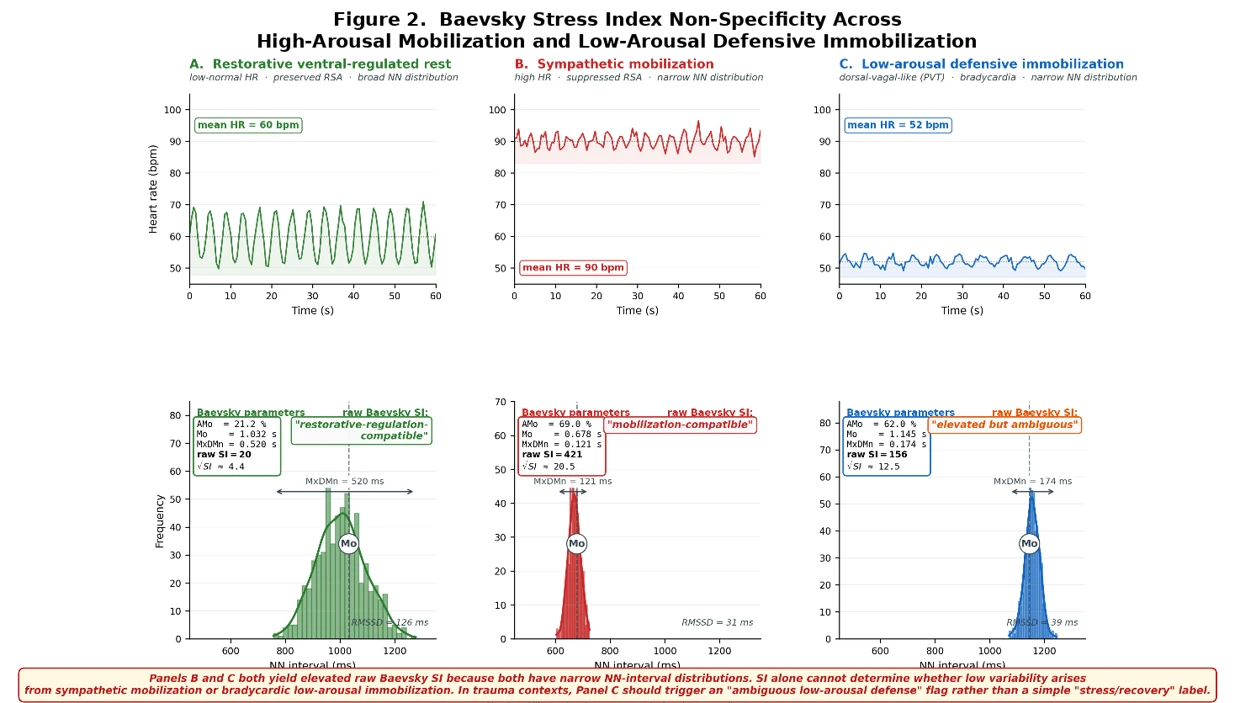
Figure 2. Baevsky Stress Index non– specificity across three simulated autonomic patterns. Top row: simulated 60 second heart rate traces. Bottom row: simulated NN-interval distributions with raw Baevsky Stress Index calculations. Panel A illustrates restorative ventral– regulated rest, with low– normal heart rate, high phasic variability, preserved respiratory– linked oscillation, broad NN distribution, and low raw SI. Panel B illustrates sympathetic mobilization, with high heart rate, reduced variability, narrow NN distribution, and high raw SI. Panel C illustrates a low-arousal defensive immobilization pattern, clinically compatible with dorsal-vagal-like shutdown in the PVT framework, with bradycardia, low variability, narrow NN distribution, and elevated raw SI. Panels B and C both yield elevated raw SI because both distributions are narrow and modal, although their heart rate levels and clinical meanings differ. The figure therefore illustrates a mathematical non-specificity of SI: without respiration, movement, blood pressure/EDA, behavioral context, and self-report, SI cannot determine whether low variability reflects high– arousal mobilization or bradycardic immobilization. Values are simulated for conceptual illustration and are not diagnostic thresholds. Kubios documentation describes Baevsky SI computation and a square root transformation; therefore this figure reports raw SI for mathematical transparency, with √SI shown for comparison.
8.2 Geometric analysis
Recall the formula:
(with AMo expressed as a percentage value, as defined in Section 3).
Three structural features of this formula combine to produce the non-specificity:
- The denominator is dominated by MxDMn (variation range). In any state of suppressed variability – whether sympathetic or defensive – MxDMn shrinks, and the SI rises sharply.
- The numerator scales with AMo (mode amplitude). When the NN-interval distribution becomes peaked and modal – again, in any state of suppressed variability –AMo rises, further increasing the SI.
- The Mo (modal NN) appears in the denominator linearly. This is the only term that partially counteracts the SI elevation in defensive immobilization: a long Mo (low HR) makes the denominator larger and the SI smaller. However, this partial counteraction is mathematically dominated by the AMo and MxDMn effects when variability is sufficiently suppressed.
The result, as shown in Figure 1, is that defensive immobilization (panel C) produces a raw Stress Index of approximately 156 – five to ten times higher than restorative regulation. This raw SI is lower than that of full sympathetic mobilization (≈421) but is unambiguously elevated above resting baseline, and would often invite a stress interpretation if read outside the broader bradycardic, behavioral, and clinical context. We propose the term Baevsky paradox for this potential misclassification: a raw SI elevation driven by NN-interval compression may be interpreted as sympathetic stress even when the broader physiological pattern is bradycardic and low-arousal.
Therefore, the problem is not that Baevsky SI is mathematically wrong. It does what it is designed to do: it detects concentration and compression of the NN-interval distribution. The problem arises when this geometric compression is interpreted as sympathetic stress without considering heart rate level, respiration, movement, blood pressure, electrodermal activity, clinical state, and self-report.
In Kubios's SNS Index pipeline, this elevated raw Baevsky SI contributes positively to a sympathetic– state output, while the simultaneous bradycardia (low mean HR) contributes negatively. The composite SNS Index is therefore an unstable output of competing signals. In Kubios's PNS Index pipeline, the long mean NN contributes positively to a parasympathetic state output, while the suppressed RMSSD and SD1 contribute negatively. The composite PNS Index is similarly unstable.
The proprietary weighting of these components determines which signal dominates in the final output. The crucial point is that this output cannot, in principle, distinguish defensive immobilization from any other state. The algorithm's output space contains only two categories; the physiology has at least three.
8.3 Why this is structural, not parametric
It is important to be clear that this is not a calibration problem. Re– tuning the weighting coefficients of the Baevsky SI, or adjusting normative reference values, cannot resolve the issue. When both sympathetic mobilization and defensive immobilization produce narrow NN– interval distributions, both drive the Baevsky SI component upward. Re– weighting the composite cannot infer the physiological origin of that compression from SI alone. The only way to distinguish them is to add information that the binary model does not represent – for example, the joint pattern of HR and HRV, respiratory entrainment, movement, and contextual or subjective state.
This is the strongest formulation of the central thesis: the blind spot is not a failure of HRV measurement; it is a failure of autonomic state ontology. Current algorithms can detect low variability, but they cannot determine whether bradycardic low variability reflects recovery, mobilization-related strain, or low-arousal defensive immobilization without additional respiratory, behavioral, contextual, and subjective data.
- A Three– State Interpretive Framework
A trauma-informed interpretation of HRV and wearable data should distinguish at least three functional autonomic states.
|
State |
Heart rate |
HRV / RSA |
Breathing |
Movement |
Subjective / clinical context |
|
Restorative regulation / safety |
Low–normal |
Normal or high relative to baseline |
Stable, flexible, non– suppressed |
Low but relaxed |
Safety, connection, rest, recovery |
|
Sympathetic mobilization |
High or rising |
Low |
Faster, irregular, effortful |
Increased or tense |
Alarm, vigilance, anger, fear, effort |
|
Low– arousal defensive immobilization |
Low, falling, or unusually flat |
Low, rigid, or flattened |
Shallow, suppressed, irregular, or overly fixed |
Very low, frozen, collapsed |
Numbness, dissociation, helplessness, shutdown, collapse |
The key clinical distinction is between restorative low arousal and defensive low arousal. Current wearable and HRV systems are generally better at detecting mobilization than immobilization, and they are generally unable to differentiate restorative from defensive patterns of low arousal.
The framework can be articulated in polyvagal language for clinical communication, but its empirical foundation does not require polyvagal anatomical specification. It rests on:
- The well–established psychophysiology of freezing and defensive bradycardia (Hashemi et al., 2019; Niermann et al., 2017; Roelofs, 2017).
- The clinical phenomenology of trauma-related dissociation and shutdown (Beutler et al., 2022; Schauer & Elbert, 2010).
- The recognized heterogeneity of autonomic configurations in PTSD and complex trauma (Kozlowska et al., 2015; Perry, 2006, 2014; Powers et al., 2021; van der Kolk, 2014).
- Preliminary Proposal: Low-Arousal Defensive State Index (LADSI)
Future wearable and HRV systems should not report only stress and recovery. They should also estimate whether a low–arousal state is likely to be restorative or defensive. We propose, as a preliminary research construct, a Low–Arousal Defensive State Index (LADSI) built from multimodal indicators.
10.1 Candidate components
- Heart rate below personal daytime baseline, or abrupt heart– rate deceleration episodes.
- RMSSD, SD1, or respiratory– linked HRV below personal baseline.
- Reduced RSA amplitude relative to breathing rate (i.e., flattened cardiopulmonary coupling), interpreted only when respiration is monitored directly.
- Very low movement outside scheduled sleep or intentional rest (e.g., during waking hours or post– exposure to a known trigger).
- Shallow, suppressed, irregular, or unusually rigid breathing.
- Optional physiological channels: electrodermal activity (EDA), blood pressure, peripheral temperature, pulse oximetry, postural sway.
- Subjective markers: numbness, detachment, collapse, derealization, depersonalization, helplessness, fatigue.
- Contextual markers: trauma trigger, interpersonal threat, post– session collapse, shutdown episode, dissociative episode.
10.2 Functional role
LADSI should not be diagnostic. It should function as a probabilistic clinical flag attached to existing wearable outputs:
“Low physiological stress score may be unreliable here. The pattern may reflect low– arousal defensive immobilization rather than recovery.”
This functions as an interpretive corrector rather than a replacement for existing scores. It preserves the value of current platforms while addressing the missing state explicitly.
10.3 Why a flag rather than a category
We deliberately propose LADSI as a flag rather than as a fourth output category for several reasons. First, defensive immobilization is heterogeneous and may not have a single canonical signature (Beutler et al., 2022). Second, the contextual and subjective components of LADSI (criteria 7 and 8) cannot be fully captured by passive sensors and require integration with patient – reported data or clinical input. Third, the conservative scientific framing favored throughout this paper – that algorithms are not "wrong" but interpretively incomplete – is best served by an additive rather than competing construct.
- Clinical Implications
The clinical consequences of the missing third state are significant.
First, patients may feel collapsed, numb, or dissociated while their device suggests low stress or acceptable recovery. This can invalidate the patient's experience and erode interoceptive trust – the very capacity that trauma therapy seeks to restore (Levin et al., 2021; Levine et al., 2018; Manolova & Vezenkov, 2025a, 2025b; Payne et al., 2015, 2015; Perry, 2006, 2009, 2014; Thayer et al., 2009; Thayer & Lane, 2009; van der Kolk, 2014; Vezenkov & Manolova, 2026). We use the term algorithmic invalidation – or, in patient language, algorithmic gaslighting – to describe the clinical experience in which device feedback repeatedly contradicts the patient's embodied state. The terminology is offered as a clinical descriptor, not a polemical claim about manufacturer intent.
Second, therapists may overvalue HRV scores without considering breathing, medication, illness, sleep stage, dissociation, trauma cues, and subjective safety. The score appears authoritative; the qualification "this is a recovery estimate, not a state classifier" is rarely surfaced in user facing materials.
Third, patients may be encouraged to "trust the device" over interoception. In trauma therapy this is risky, because a central clinical task is precisely to distinguish safety from collapse.
Fourth, a device score may unintentionally reinforce shame or self-doubt: "My watch says I am fine, but I feel terrible." That mismatch is not trivial. It is clinically meaningful and may be a useful entry point for psychoeducation, but it requires that the clinician understand the structural source of the mismatch.
Fifth, in early phases of effective trauma therapy – when patients begin to mobilize out of shutdown – device reported recovery scores may transiently worsen, which can be misread by the patient as deterioration. Without clinical contextualization, this can undermine treatment adherence.
A trauma– informed interpretation of wearable data should include explicit framing such as:
- Your device measures signals, not meaning.
- Low stress on the watch does not necessarily mean safety.
- Low heart rate can occur in recovery, but also in shutdown.
- Low HRV can reflect stress, illness, fatigue, rigidity, or dissociation.
- We interpret the data together with your body experience and context.
These framings can be included in psychoeducation and in clinician training in trauma– focused settings where wearables are increasingly used as adjuncts to therapy.
- Implications for the Peer– Reviewed Literature
The implications extend beyond clinical practice. Kubios-derived indices – PNS Index, SNS Index, and Stress Index – are increasingly used to characterize autonomic function in published research on trauma-exposed, dissociative, chronically fatigued, and psychiatrically ill samples. A representative subset of this literature describes findings such as "elevated stress index" or "reduced PNS index" in clinical groups, often interpreted as evidence of sympathetic hyperactivation or parasympathetic suppression.
The argument developed in Sections 7 and 8 implies that these interpretations may be physiologically incomplete for a subset of participants whose clinical state is one of low-arousal defensive immobilization rather than sympathetic mobilization. Specifically:
- An "elevated SNS Index" driven primarily by an elevated raw Baevsky SI in a sample with bradycardia and reduced overall HRV may reflect compression of the NN– interval distribution from variability suppression, not sympathetic activation.
- A "reduced PNS Index" in such a sample may reflect loss of high frequency cardiac modulation without distinguishing this from the simpler interpretation of "low parasympathetic tone."
- Group– level comparisons that find "stress" in clinical samples may be combining heterogeneous autonomic states (some sympathetic, some defensive) under a single label.
This is a hypothesis, not a proven empirical finding. It suggests that re-analysis of existing datasets with attention to the three state framework could yield substantively different physiological interpretations. At minimum, future studies using Kubios-derived composite indices in trauma-exposed samples should report the underlying parameters (mean NN, RMSSD, SD1, SD2, raw Baevsky SI, MxDMn, AMo) separately, allowing readers to evaluate whether the composite indices may be confounded.
This recommendation aligns with the broader call by Billman (2013) and others for HRV researchers to move beyond composite metrics toward direct reporting of physiologically meaningful parameters, alongside contextual variables sufficient for state inference.
- Research Agenda
The next step is empirical validation of the three– state framework and of LADSI as a useful interpretive flag.
13.1 Participants
A suitable study would enroll several groups:
- Complex trauma patients with predominantly hypoarousal/dissociative presentations.
- PTSD patients with and without dissociative subtype.
- Patients with shutdown/freeze presentations (clinically identified by experienced trauma clinicians).
- Healthy controls.
- Endurance– trained controls (an essential comparison group). Highly trained athletes commonly present with low resting heart rate combined with high HRV – the prototypical signature of restorative regulation. Comparing this group with trauma patients showing low HR + low HRV directly tests whether existing algorithms can distinguish restorative bradycardia from defensive bradycardia.
13.2 Physiological data
- Polar watch data: Nightly Recharge components, ANS Charge, heart rate, HRV, breathing rate, sleep estimates.
- Polar H10 or research-grade ECG-derived NN intervals (for ground– truth validation of PPG-based metrics).
- Kubios-derived RMSSD, SD1, SD2, raw Baevsky SI, square root SI, PNS Index, SNS Index.
- Direct respiration measurement (respiration belt or validated estimate from ECG-derived respiration).
- Continuous or intermittent blood pressure.
- Peripheral temperature.
- Movement and postural sway (accelerometry, force plate where available).
13.3 Clinical and subjective data
- Momentary subjective safety ratings.
- Subjective stress ratings.
- Dissociation ratings (e.g., DES-II state version, or items from the Multidimensional Inventory of Dissociation).
- Numbness / collapse / fatigue ratings.
- Trigger context.
- Session timing and post– session monitoring.
- Therapist– rated autonomic state observations.
- Ecological momentary assessment across days.
13.4 Primary hypothesis
A subgroup of trauma patients will show:
- low heart rate + low HRV/RSA + low movement + subjective numbness/dissociation/collapse
while wearable or HRV-derived stress/recovery models classify the pattern as low stress, recovery, poor recovery, or ambiguous strain rather than as low-arousal defensive immobilization. The misclassification rate will exceed that of a multimodal LADSI-style classifier incorporating respiration, movement, subjective state, and context.
13.5 Secondary hypotheses
- The endurance trained group and the defensive immobilization group will be reliably distinguishable by respiration corrected RSA amplitude and cardiopulmonary phase coupling, even when mean HR and RMSSD are similar.
- The raw Baevsky Stress Index will show systematically elevated values in the defensive immobilization group despite bradycardia, providing empirical support for the geometric analysis in Section 8.
13.6 Methodological recommendations
- Reporting standards: studies should report all individual level Baevsky parameters (Mo, AMo, MxDMn) alongside any composite SI values, and should distinguish raw SI from square root SI.
- Statistical analysis: composite indices should not be compared across groups without parallel reporting of components, to allow detection of confounded patterns.
- Sample stratification: trauma samples should be stratified by predominant presentation (hyperarousal vs. hypoarousal/dissociative) before HRV analysis, given the heterogeneity established in the literature (Beutler et al., 2022).
- Limitations
This paper does not claim that Polar, Kubios, or other systems are technically invalid. Polar's Nightly Recharge is a recovery model designed for general adult populations, and Kubios HRV Scientific is a rigorous HRV analysis platform widely validated in research settings. The claim is narrower: these systems should not be used as standalone classifiers of trauma– related autonomic states.
This paper also does not claim that HRV directly measures ventral or dorsal vagal activity. RSA, RMSSD, SD1, and the Baevsky SI are useful but indirect and context sensitive markers. The paper uses polyvagal language cautiously, as a clinical state model with face validity for trauma-informed practice, while acknowledging that key physiological claims of polyvagal theory remain disputed (Grossman et al., 2026). The central argument – that a third autonomic state of low-arousal defensive immobilization is missing from current algorithmic output ontologies – does not require resolution of the polyvagal debate.
The geometric analysis in Section 8 uses illustrative simulated data to make a structural mathematical point. Empirical validation in real clinical populations (Section 13) is required before any specific quantitative claim about the prevalence or magnitude of misclassification can be made.
We also note that we have not directly examined every Kubios output mode or every Polar feature; new versions of these platforms may include additional analyses or contextual flags not discussed here. The structural argument applies to the public composite outputs as currently described in manufacturer documentation.
The proposed LADSI construct should not be interpreted as a validated measure of dorsal vagal activity or dissociation. It is a hypothesis generating interpretive flag intended to identify cases in which existing stress/recovery scores may be clinically underdetermined. Its value must be tested against multimodal physiological data, clinician rated state, and patient reported experience.
Finally, low– arousal defensive immobilization itself requires better empirical definition. Trauma– related dissociation does not show one universal autonomic signature (Beutler et al., 2022). This is precisely why multimodal and context sensitive models – and a flag-based rather than category-based interpretive correction – are needed.
- Conclusion
The central problem in wearable and HRV-based stress interpretation is not only measurement accuracy. It is the absence of a sufficient autonomic state ontology.
Polar and Kubios provide valuable physiological data. Polar can estimate overnight recovery relative to personal baseline. Kubios can quantify HRV, rhythm variability, raw and square root Baevsky SI, and PNS/SNS-related composites. But neither system, by itself, can determine whether low heart rate, low HRV, low RSA, and low movement indicate recovery, mobilization, or low-arousal defensive immobilization. The geometric structure of the Baevsky Stress Index in particular makes such discrimination structurally limited: defensive immobilization and sympathetic mobilization both produce narrow NN-interval distributions, both yield elevated raw SI values, and both contribute non– trivially to composite "stress" outputs regardless of weighting.
The blind spot is not a failure of HRV measurement; it is a failure of autonomic state ontology. Current algorithms can detect low variability, but they cannot determine whether bradycardic low variability reflects recovery, mobilization– related strain, or low– arousal defensive immobilization without additional respiratory, behavioral, contextual, and subjective data.
In trauma– informed practice, this distinction is not optional. It is clinically essential.
The argument does not require accepting every claim of polyvagal theory. Even on the most conservative reading of the recent expert critique (Grossman et al., 2026), the freezing literature alone (Roelofs, 2017) establishes that low-arousal defensive states with cardiac deceleration are real, common, and clinically distinct from rest. The gap is not theoretical but ontological: current algorithms have two output categories, and the physiology has at least three.
Trauma– informed autonomic interpretation requires at least three functional categories: restorative regulation, sympathetic mobilization, and low-arousal defensive immobilization. Current HRV-based stress/recovery outputs generally represent the first two more clearly than the third.
The future of wearable psychophysiology should not be merely more accurate sensors. It should be better state interpretation. The Low-Arousal Defensive State Index proposed here is one preliminary route toward such models. Until validated tools are available, clinicians should treat wearable stress and recovery scores as partial physiological data, not as authoritative interpretations of the patient's nervous system.
The missing variable is not another HRV metric. The missing variable is the third autonomic state.
Disclosure Statement
The author declares no commercial conflicts of interest with respect to the manufacturers discussed in this article. The author has used Polar devices and Kubios software both personally and in clinical contexts with trauma patients, which informs the observations presented.
Ethics
This Perspective article does not report original human subjects data. No patient identifying information is included.
References
Baevsky, R. M., & Chernikova, A. G. (2017). Heart rate variability analysis: Physiological foundations and main methods. Cardiometry, (10). https://scholar.archive.org/work/6de6pr3t5bh2fbt3x74dpgsz6q/access/wayback/http://www.cardiometry.net/issues/no10-may-2017/item/download/316_88e37a72e8ffeee25c25d7665b7774d1
Beutler, S., Mertens, Y. L., Ladner, L., Schellong, J., Croy, I., & Daniels, J. K. (2022). Trauma-related dissociation and the autonomic nervous system: A systematic literature review of psychophysiological correlates of dissociative experiencing in PTSD patients. European Journal of Psychotraumatology, 13(2), 2132599. https://doi.org/10.1080/20008066.2022.2132599
Billman, G. E. (2013). The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Frontiers in Physiology, 4. https://doi.org/10.3389/fphys.2013.00026
Boudreau, P., Yeh, W.-H., Dumont, G. A., & Boivin, D. B. (2013). Circadian Variation of Heart Rate Variability Across Sleep Stages. Sleep, 36(12), 1919–1928. https://doi.org/10.5665/sleep.3230
Doherty, C., Baldwin, M., Keogh, A., Caulfield, B., & Argent, R. (2024). Keeping Pace with Wearables: A Living Umbrella Review of Systematic Reviews Evaluating the Accuracy of Consumer Wearable Technologies in Health Measurement. Sports Medicine, 54(11), 2907–2926. https://doi.org/10.1007/s40279-024-02077-2
Doherty, C., Baldwin, M., Lambe, R., Burke, D., & Altini, M. (2025). Readiness, recovery, and strain: An evaluation of composite health scores in consumer wearables. Translational Exercise Biomedicine, 2(2), 128–144. https://doi.org/10.1515/teb-2025-0001
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/S0749-3797(98)00017-8
Grossman, P. (2023). Fundamental challenges and likely refutations of the five basic premises of the polyvagal theory. Biological Psychology, 180, 108589. https://doi.org/10.1016/j.biopsycho.2023.108589
Grossman, P., Ackland, G. L., Allen, A. M., Berntson, G. G., Booth, L. C., Burghardt, G. M., Buron, J., Dinets, V., Doody, J. S., Dutschmann, M., Farmer, D. G. S., Fisher, J. P., Gourine, V., Joyner, M. J., Karemaker, J. M., Khalsa, S. S., Lakatta, E. G., Leite, C. A. C., Macefield, G., … Zucker, I. H. (2026). Why the polyvagal theory is untenable. An international expert evaluation of the polyvagal theory and commentary upon Porges, S.W. (2025). Polyvagal theory: Current status, clinical applications, and future directions. Clin. Neuropsychiatry, 22(3), 169–184. https://doi.org/10.36131/cnfioritieditore20260110
Grossman, P., & Taylor, E. W. (2007). Toward understanding respiratory sinus arrhythmia: Relations to cardiac vagal tone, evolution and biobehavioral functions. Biological Psychology, Special Issue of Biological Psychology on Cardiac Vagal Control, Emotion, Psychopathology, and Health., 74(2), 263–285. https://doi.org/10.1016/j.biopsycho.2005.11.014
Hashemi, M. M., Gladwin, T. E., de Valk, N. M., Zhang, W., Kaldewaij, R., van Ast, V., Koch, S. B. J., Klumpers, F., & Roelofs, K. (2019). Neural Dynamics of Shooting Decisions and the Switch from Freeze to Fight. Scientific Reports, 9(1), 4240. https://doi.org/10.1038/s41598-019-40917-8
Kozlowska, K., Walker, P., McLean, L., & Carrive, P. (2015). Fear and the Defense Cascade: Clinical Implications and Management. Harvard Review of Psychiatry, 23(4), 263. https://doi.org/10.1097/HRP.0000000000000065
Kubios. (2024). HRV analysis methods—How is HRV calculated. Kubios. https://www.kubios.com/blog/hrv-analysis-methods/
Levin, Y., Lev Bar-Or, R., Forer, R., Vaserman, M., Kor, A., & Lev-Ran, S. (2021). The association between type of trauma, level of exposure and addiction. Addictive Behaviors, 118, 106889. https://doi.org/10.1016/j.addbeh.2021.106889
Levine, P. A., Blakeslee, A., & Sylvae, J. (2018). Reintegrating Fragmentation of the Primitive Self: Discussion of “Somatic Experiencing.” Psychoanalytic Dialogues, 28(5), 620–628. https://doi.org/10.1080/10481885.2018.1506216
Manolova, V., & Vezenkov, S. (2025a). Screen Trauma – Specifics of the Disorder and Therapy in Adults and Children. Nootism, 1(1), 37–51. https://doi.org/10.64441/nootism.2NCSC.3
Manolova, V., & Vezenkov, S. (2025b). Unified Trauma-Addiction Functioning Model. Nootism, 1(4), 4–24. https://doi.org/10.64441/nootism.1.4.1
Niermann, H. C., Figner, B., & Roelofs, K. (2017). Individual differences in defensive stress-responses: The potential relevance for psychopathology. Current Opinion in Behavioral Sciences, Stress and Behavior, 14, 94–101. https://doi.org/10.1016/j.cobeha.2017.01.002
Payne, P., Levine, P. A., & Crane-Godreau, M. A. (2015). Somatic experiencing: Using interoception and proprioception as core elements of trauma therapy. Frontiers in Psychology, 6. https://doi.org/10.3389/fpsyg.2015.00093
Perry, B. D. (2006). Fear and learning: Trauma‐related factors in the adult education process. New Directions for Adult and Continuing Education, 2006(110), 21–27. https://doi.org/10.1002/ace.215
Perry, B. D. (2009). Examining Child Maltreatment Through a Neurodevelopmental Lens: Clinical Applications of the Neurosequential Model of Therapeutics. Journal of Loss and Trauma, 14(4), 240–255. https://doi.org/10.1080/15325020903004350
Perry, B. D. (2014). The Neurosequential Model of Therapeutics: Application of a developmentally sensitive and neurobiology-informed approach to clinical problem solving in maltreated children. In Infant and early childhood mental health: Core concepts and clinical practice (pp. 21–53). American Psychiatric Publishing, Inc.
Porges, S. W. (2025). POLYVAGAL THEORY: CURRENT STATUS, CLINICAL APPLICATIONS, AND FUTURE DIRECTIONS. Clinical Neuropsychiatry, 22(3), 175–191. https://doi:10.36131/cnfioritieditore20250301
Powers, A., Mekawi, Y., Fickenwirth, M., Nugent, N. R., Dixon, H. D., Minton, S., Kim, Y. J., Gluck, R., Carter, S., Fani, N., Schwartz, A. C., Bradley, B., Umpierrez, G. E., Pace, T. W. W., Jovanovic, T., Michopoulos, V., & Gillespie, C. F. (2021). Emotion dysregulation and dissociation contribute to decreased heart rate variability to an acute psychosocial stressor in trauma-exposed Black women. Journal of Psychiatric Research, 142, 125–131. https://doi.org/10.1016/j.jpsychires.2021.07.032
Roelofs, K. (2017). Freeze for action: Neurobiological mechanisms in animal and human freezing. Philosophical Transactions of the Royal Society B: Biological Sciences, 372(1718), 20160206. https://doi.org/10.1098/rstb.2016.0206
Schauer, M., & Elbert, T. (2010). Dissociation Following Traumatic Stress. Zeitschrift Für Psychologie / Journal of Psychology, 218(2), 109–127. https://doi.org/10.1027/0044-3409/a000018
Shaffer, F., & Ginsberg, J. P. (2017). An Overview of Heart Rate Variability Metrics and Norms. Frontiers in Public Health, 5, 258. https://doi.org/10.3389/fpubh.2017.00258
Thayer, J. F., Hansen, A. L., Saus-Rose, E., & Johnsen, B. H. (2009). Heart Rate Variability, Prefrontal Neural Function, and Cognitive Performance: The Neurovisceral Integration Perspective on Self-regulation, Adaptation, and Health. Annals of Behavioral Medicine, 37(2), 141–153. https://doi.org/10.1007/s12160-009-9101-z
Thayer, J. F., & Lane, R. D. (2009). Claude Bernard and the heart–brain connection: Further elaboration of a model of neurovisceral integration. Neuroscience & Biobehavioral Reviews, 33(2), 81–88. https://doi.org/10.1016/j.neubiorev.2008.08.004
van der Kolk, B. A. (2014). The body keeps the score: Brain, mind, and body in the healing of trauma (pp. xvi, 443). Viking.
Vezenkov, S., & Manolova, V. (2026). Screen Addiction in Children and Adults: Biomarkers, Screen Trauma and Reversed Development. Nootism, 2(1), 4–45. https://doi.org/10.64441/nootism.2.1.1