Martin I. Mateev, Iveta H. Pashina, Violeta R. Manolova, Stoyan R.Vezenkov
Center for applied neuroscience Vezenkov, BG-1582 Sofia, e-mail: info@vezenkov.com
For citation: Mateev M.I., Pashina I.H., Manolova V.R. and Vezenkov S.R. (2025) Restoring Neural Coherence Through Screen Addiction Therapy in a 12-Year-Old with Autism Spectrum Disorder: Case Report. Nootism 1 (3), 27-33, ISSN 3033-1765 (print), ISSN 3033-1986 (online) https://doi.org/10.64441/nootism.1.3.4
Abstract
This case study explores the therapeutic outcomes of a five-month multimodal intervention in a 12-year-old boy with a diagnosis of atypical autism and a long-standing history of early-onset screen addiction and screen-induced trauma. The intervention included a complete digital detox, sensory and motor integration training, and systemic family therapy. Quantitative EEG (qEEG) assessments were conducted pre- and post-intervention to evaluate changes in neural coherence patterns.
The results demonstrated significant improvements in behavioral regulation, emotional responsiveness, sensorimotor functioning, and social engagement. qEEG analysis revealed marked reductions in cortical hypercoherence, particularly in the beta frequency bands (12–25 Hz), and partial normalization of interhemispheric coherence, especially in the eyes-open condition. However, coherence abnormalities in the occipital cortex persisted, and the child experienced episodic regressions, sleep instability, and vulnerability to environmental stressors.
This case highlights the neuroplastic potential of late interventions in screen-induced neurodevelopmental disruptions, while also underscoring the limitations of therapy initiated beyond early childhood. The findings underscore the importance of early detection and intensive, immersive intervention strategies to facilitate cortical reorganization in children with screen addiction and a diagnosis of Autism Spectrum Disorder.
Keywords: screen addiction, autism spectrum disorder, EEG coherence, neurotherapy, child development, digital detox, interhemispheric synchronization
Introduction
One of the essential questions we face in the therapy of early-onset screen addiction in children with Autism Spectrum Disorder (ASD) is: after what age is full recovery no longer achievable? What are the prognostic outcomes of therapy initiated after the age of nine?
In several of our previous studies, we have published results from a comprehensive therapeutic approach (Vezenkov et al., 2025 (1)(2); Pashina et al., 2025; Petrov et al., 2025; Petkova et al., 2025) that involves the entire family and addresses both the screen addiction and the resulting functional impairments in the child (Vezenkov et al., 2025 (3)).
In our first documented case—a 12-year-old nonverbal girl with ASD, marked by severe automatisms, compulsions, stereotypic behaviors, intense screen addiction, and screen-induced trauma—we observed remarkable results after nine months of therapy (Manolova et al., 2025 (1)). Screen addiction was entirely eliminated, and many autistic traits significantly diminished. However, the therapy ultimately failed at the parental level—particularly with the mother, who terminated the process after prolonged resistance and sabotage (Vezenkov et al., 2024). This case introduced us to a new phenomenon: Munchausen Syndrome by Proxy, which we subsequently described in detail (Manolova et al., 2025 (2)).
In this article, we describe the case of another 12-year-old child—a boy with early-onset screen addiction, screen trauma, and an ASD diagnosis. To what extent can recovery be achieved through our therapeutic model after such a prolonged history of screen addiction and associated trauma?
Study Design
A quasi-experimental design was employed, incorporating pre- and post-intervention measurements targeting screen addiction and screen-induced trauma.
Comprehensive Family Therapy
The conceptual framework underlying the implemented comprehensive therapeutic approach has been described in prior publications (Vezenkov et al., 2024 (1); (2); 2025 (1); (2); Manolova et al., 2025 (1)). This model integrates family-based intervention strategies that address both the child's condition and the systemic family dynamics contributing to screen dependency.
qEEG Assessment
Electroencephalographic (EEG) recordings were conducted using a 19-channel monopolar montage, implemented via the Neuron-Spectrum-4P system and Neuron-Spectrum.NET software (Neurosoft LLC, Russia). Quantitative spectral analysis—comprising amplitude evaluation across various frequency bands and other electrophysiological indicators—was performed within Neuron-Spectrum.NET.
For normative comparisons, quantitative EEG parameters (including absolute and relative amplitudes, coherence, phase lag, and Z-scores) were further analyzed using NeuroGuide Deluxe 3.3.0 (Applied Neuroscience, Inc., USA), referencing a validated normative neurodatabase.
Case History
For functional assessment, a 12-year-old boy named Adam (pseudonym) was brought to the Center by his mother. He had been diagnosed with Autism Spectrum Disorder (atypical autism) at the age of five by a clinical psychologist. Following the diagnosis, he underwent three years of occupational therapy and Applied Behavior Analysis (ABA) therapy.
Adam presented with severe automatisms, compulsive and stereotypical hyperactive behaviors, and was nonverbal. He exhibited automatic speech, used out of context and not for social interaction. He appeared to suffer from frequent, possibly severe headaches, often clutching his head and crying.
Up until the age of six, Adam experienced severe sleep disturbances, characterized by persistent insomnia and continuous crying throughout the night. Some improvement was noted thereafter. He habitually fell asleep while watching videos on a phone. If awakened during the night, he was unable to fall back asleep.
His eating difficulties included selective food intake, with a complete refusal of raw vegetables. Up to the age of nine, he experienced chronic diarrhea, which later resolved. Until the age of five, he consumed only pureed food and lacked the ability to chew. Feeding was always conducted in front of a screen.
Adam exhibited deficits in self-care abilities and required assistance for routine daily activities, although he was able to feed himself independently. Following intensive therapy, he acquired new skills such as riding a bicycle, swimming, and wall climbing. He continued to avoid social interaction with peers and was supported by a personal assistant in his daily life.
According to his mother, Adam had been exposed to television from the age of six months, as her high-responsibility public service position did not allow for sufficient maternal care. At the time of the assessment, his daily screen time averaged approximately four hours.
The Screen-Induced Post-Visual Reactivity (SIPVR) test was positive, showing a severe reaction, including eye-covering behavior (Vezenkov et al., 2025 (3)). Upon completion of all diagnostic procedures, Adam was found to exhibit a severe form of screen addiction.
Indicators of screen-induced trauma were clearly identifiable in the EEG recordings, which displayed characteristic splitting and fragmentation patterns, as well as slow-wave episodes in the 5–6 Hz frequency range—hallmarks of severe screen-related neurophysiological disruption.
Results
Key Highlights During Therapy
At the outset of therapy, Adam’s mother presented with a distressed emotional profile, characterized by anxious-depressive symptoms, persistent apathy, and a marked absence of pleasure or recreational engagement. She suffered from chronic insomnia, migraines, and hormonal imbalance. Her daily routine included evening alcohol consumption—typically two glasses of wine. The family dynamic was limited: she had an adult daughter (25+) living independently, and her social circle was restricted to her mother and daughter. Adam’s father had withdrawn from parental responsibilities when Adam was two years old and was now part of a separate family. He had minimal contact with Adam and was generally absent from caregiving. The mother expressed no interest in forming new romantic relationships and actively avoided interactions with men.
After the removal of screen exposure, Adam became significantly calmer, began to sleep well, but started experiencing upper respiratory infections—a new development, as he had not been ill for years. The first signs of withdrawal symptoms also emerged. Despite this, Adam did not exhibit screen-seeking behaviors, nor did he experience tantrums, crises, or aggressive outbursts, much to his mother’s surprise, as she had anticipated and feared such reactions.
By the third week of therapy, Adam began to try new foods, seek proximity to his mother, and became hyperexcited during play with her. As a result, he had increased difficulty falling asleep in the evenings.
By the fourth week, Adam's sleep pattern shifted again: he began going to bed at 10:00 PM and waking around 4–5:00 AM, yet appeared alert and in a good mood upon waking. Both therapists and the school resource teacher reported significant positive behavioral changes. Adam was cooperative and engaged in all assigned activities.
Adam’s mother also began to sleep better, attributing the improvement to the alleviation of abdominal pain she had initially experienced. This relief followed targeted biofeedback neurotherapy exercises. During the first 15 minutes of each session—up to week five—her heart rate averaged 100 bpm, which dropped to 75 bpm by the middle and end of the session.
After four weeks of therapy, her heart rate variability (HRV) parameters showed notable improvement. She also reported that neck pain and tension in the masticatory muscles had resolved. Additionally, she discontinued evening alcohol consumption.
During this period, Adam saw his father for the first time since therapy began. However, in the fifth week, a regression was observed: Adam became agitated, engaged in continuous automatic speech, and his sleep deteriorated. The SIPVR test was again positive, suggesting possible re-exposure to screens.
Adam’s mother was uncertain whether the father had allowed screen use, though he denied it. Given his history of deception and concealment, she suspected a potential screen relapse, which may have triggered the regression (Petrova et al., 2025; Vezenkov et al., 2025 (3)).
In the sixth week, following the intensification of therapeutic exercises, Adam’s sleep improved once again. For the first time, his mother began to implement the changes encouraged by the neurotherapist. She started performing her exercises regularly, engaged in physical activity, took daily walks, and shifted her focus from being solely child-centered to also attending to her own well-being.
During weeks seven and eight, Adam became increasingly restless, and his sleep quality declined again. A series of crises followed the intensive sensory restart and cortical activation exercises. The mother, feeling exhausted, finally sought additional support to assist with taking Adam to school and sports activities. She also noted a pattern: Adam tended to become agitated and had difficulty falling asleep in the two days leading up to each therapy session.
Nearly every week, fluctuations were observed in Adam’s sleep quality, behavior, and overall condition. Periods of improvement alternated with short-term crises lasting several days.
By the ninth week, only a single, short-lived episode of crisis occurred. Adam’s sleep improved notably—he woke once at 3:00 AM but managed to fall back asleep, which marked a first since the start of therapy. He began trying new foods, exploring new activities, and showed a heightened level of curiosity, actively observing his surroundings.
His mother, in parallel, appeared more energized, balanced, and emotionally uplifted. The typical correlation previously described in the dynamic between the mother's and child’s states (Pashina et al., 2025) was again evident in this case.
By week 12, Adam’s progress had become noticeably more stable. He appeared calm and quiet, with no observed crises. He met with his father for the second time since the start of therapy. Meanwhile, his mother reported continued emotional distress related to her separation from the father—despite previously believing she had moved on. At school, staff expressed high satisfaction with Adam’s improvement.
In week 13, Adam fell ill again. By week 14, after recovering, he met with his father once more. His mother reported feeling more at ease, as the father was gradually becoming more involved, encouraged by the visible progress in Adam’s development.
During weeks 18 and 19, a new regression occurred, characterized by behavioral crises, headaches, and increased episodes of automatic vocalizations. Despite this setback, Adam continued to engage in imitative behaviors, emotional expression, and social interaction—notably seeking contact with his father.
Results After Five Months of Therapy
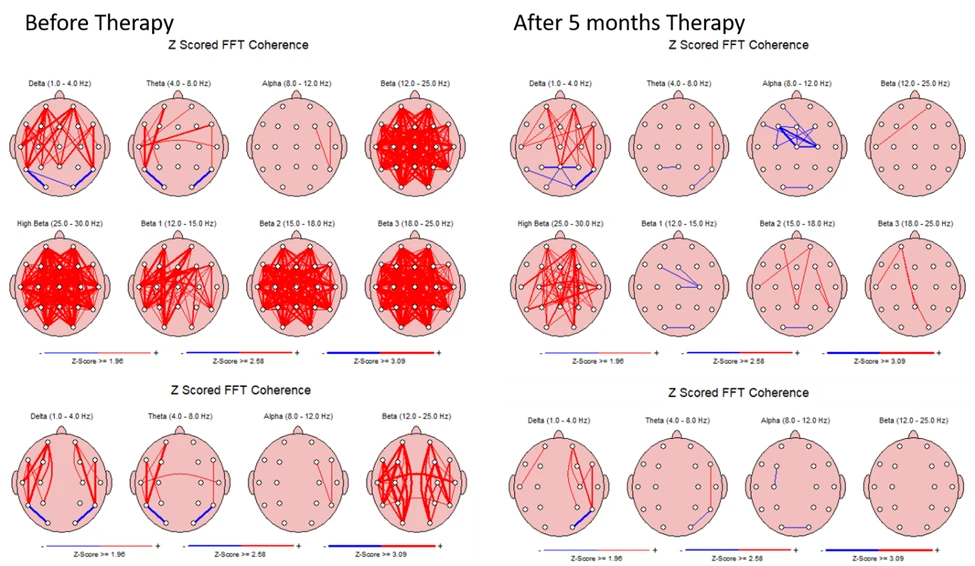
A comparative analysis of neural coherence with eyes open, conducted before and after the five-month therapeutic intervention, is presented in Figure 1.
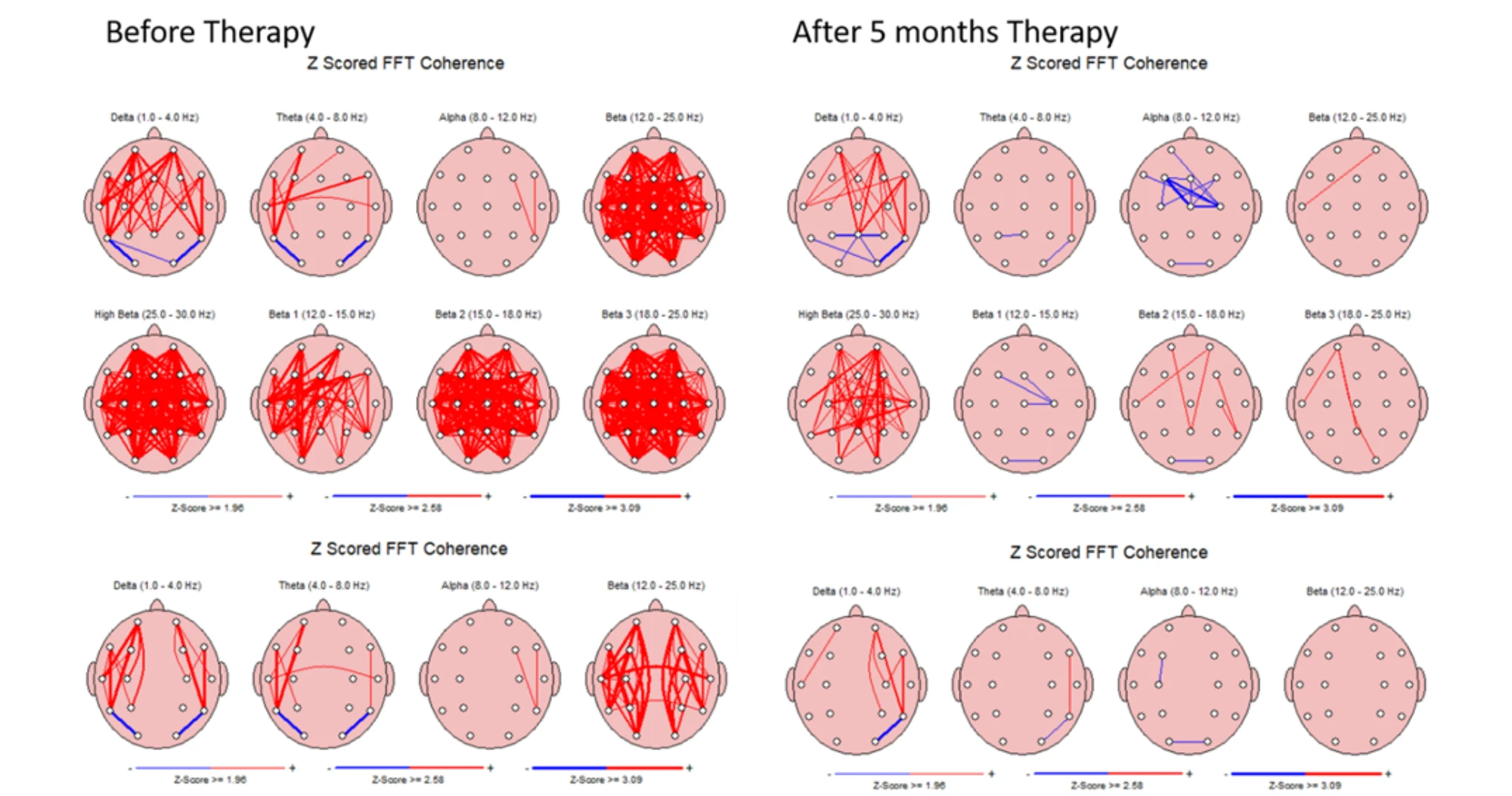
Figure 1. Neural coherence (eyes open) across different frequency bands before and after five months of therapy for screen addiction.
Figure 1 presents Z-scored FFT coherence maps across various EEG frequency bands (eyes open), comparing pre- and post-intervention data following a five-month therapy program targeting screen addiction.
Prior to therapy, the child exhibited widespread hypercoherence, particularly in the Beta 1 (12.0–15.0 Hz), Beta 2 (15.0–18.0 Hz), and Beta 3 (18.0–25.0 Hz) bands. These were marked by dense inter-electrode connectivity, as visualized by the red lines in the top panels of Figure 1. This hyperconnectivity, distributed across nearly all electrode pairings, is consistent with patterns of cortical hyperarousal, dysregulated executive function, and sensory overstimulation, commonly seen in children with neurodevelopmental disorders and screen overexposure.
Following the intervention, the coherence in Beta 1, 2, and 3 bands decreased significantly, indicating a shift toward more regulated cortical communication. The most notable improvement was the transition from generalized hypercoherence to near-normative coherence values. However, in the High Beta range (25.0–30.0 Hz), while a clear reduction was observed, coherence levels remained elevated above normative thresholds, suggesting ongoing residual cortical overstimulation.
In the Alpha band (8.0–12.0 Hz), post-therapy data showed a reduction in coherence between central and frontal regions. This may reflect enhanced functional specialization and decreased pathological coupling in regions critical for self-regulation and attention.
Minor but positive changes were also seen in the Theta band (4.0–8.0 Hz), pointing to gradual improvements in subcortical-cortical integration and early-stage processing.
A particularly important finding was the normalization of interhemispheric coherence. Before therapy, the child exhibited significantly elevated interhemispheric synchronization, which decreased to near-typical levels post-intervention. This suggests improved hemispheric balance and cognitive-emotional integration—a key therapeutic milestone.
A comparative analysis of neural coherence with eyes closed, before and after therapy, is presented in Figure 2.
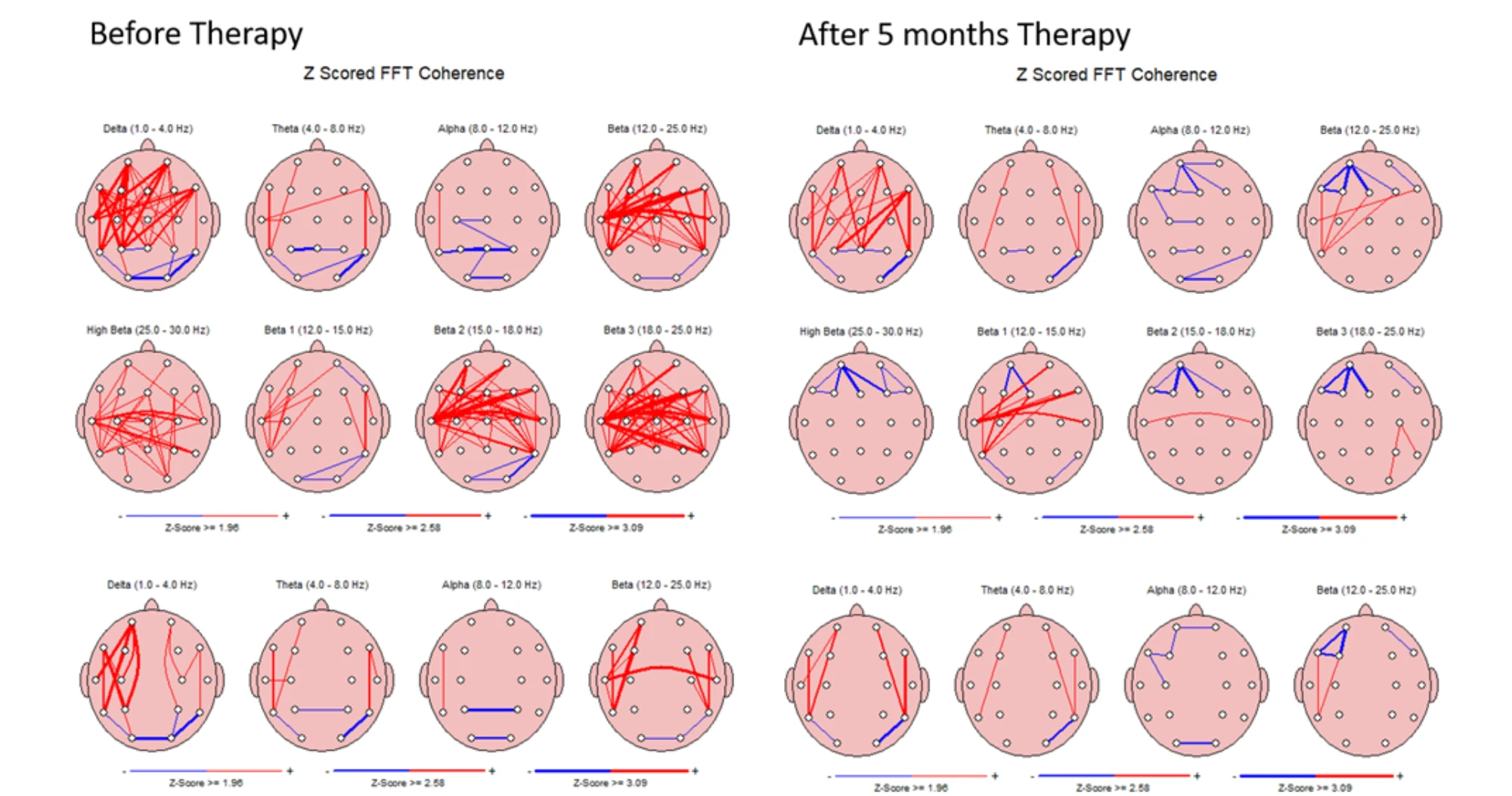
Figure 2. Neural coherence (eyes closed) across different frequency bands before and after five months of therapy for screen addiction.
Figure 2 illustrates Z-scored FFT coherence with eyes closed across different EEG frequency bands, comparing data before and after five months of therapy for screen addiction.
The most significant changes were again observed in the Beta 2 (15.0–18.0 Hz), Beta 3 (18.0–25.0 Hz), and High Beta (25.0–30.0 Hz) bands. Initially elevated coherence in these ranges—reflecting hyperconnectivity and cortical overarousal—was notably reduced post-therapy, approaching normative levels. These changes are consistent with those observed in the eyes-open condition, indicating generalized improvement in cortical regulation.
There was a clear decrease in coherence between left frontal and prefrontal regions, particularly within both the Beta and Alpha (8.0–12.0 Hz) frequency bands. This reduction may reflect improved differentiation of executive and self-regulatory networks, often overcoupled in children with ASD and screen-related dysregulation.
Despite the overall trend toward normalization, specific coherence anomalies in the occipital (visual) cortex persisted, suggesting that therapeutic effects on visual processing networks may require a longer intervention period or targeted strategies.
Discussion
The process of recovery in this case—a 12-year-old child with early-onset screen addiction and severe screen-induced trauma—was marked by significant challenges. The therapeutic course, which included a complete digital detox, was accompanied by withdrawal crises and periods of regression. Similar to other cases, the onset of therapy triggered frequent illnesses and fluctuations in sleep patterns, highlighting the disruption of the child’s previous behavioral and neurological "homeostasis", which had been artificially maintained through external regulators such as screens.
The normalization of hypercoherence in the eyes-open condition, which was more pronounced than in the eyes-closed state, suggests that the therapy was particularly effective in the active, task-related beta ranges. This pattern indicates restoration of more balanced and functional cortical communication, especially during wakeful and engaged mental states. Improvements in alpha and theta coherence were also observed, although to a lesser extent, pointing to partial reorganization in relaxation and integrative processing networks.
The observed hypercoherence—particularly interhemispheric—prior to therapy is consistent with findings associated with immature neural organization. Excessive interhemispheric coherence is considered a marker of underdeveloped hemispheric specialization and reduced functional asymmetry, traits typical of early developmental stages (Alexandrov et al., 2025; Manolova et al., 2025 (1)). The reduction in these patterns post-therapy indicates a progression toward more mature, lateralized brain function—a desirable therapeutic outcome.
Accumulating evidence points to specific EEG patterns that are strongly associated with executive functioning, especially in contexts involving working memory, attention, and decision-making. Research by Sauseng et al. (2005; 2010) highlights the critical role of fronto-parietal networks, particularly through the modulation of theta and upper alpha band activity, in supporting central executive processes.
Stronger interregional phase coherence at theta frequency—especially between frontal and temporal regions—has been linked to the integration of complex memory features and attentional control. Additionally, executive task engagement is often marked by a decrease in short-range anterior alpha connectivity and a corresponding increase in long-range fronto-parietal coherence, reflecting the dynamic recruitment of a functional fronto-parietal control network.
These findings support the hypothesis that qEEG can capture functional signatures of executive performance, providing a non-invasive window into the cognitive state of individuals under varying task demands.
EEG coherence—defined as the degree of synchronization between electrical signals recorded at different brain regions—has been widely recognized as a marker of functional connectivity and cognitive integration. High coherence, particularly within the theta (4–7 Hz), alpha (8–12 Hz), and beta (13–24 Hz) frequency bands, has been consistently associated with enhanced executive functioning, especially in tasks involving working memory, attentional regulation, and decision-making.
Greater long-range coherence in the theta band between anterior and posterior brain regions is linked to increased working memory load, while interhemispheric coherence—especially between the left and right frontal areas—has been shown to reflect efficient cognitive control processes.
Furthermore, decreased short-range coherence in anterior alpha and beta bands, accompanied by increased long-range fronto-parietal connectivity, appears to reflect the neural dynamics of flexible executive control. These patterns align with evidence from a large-scale study by (Sadaghiani et al., 2019), which confirmed that coherence in frontal regions across theta, alpha, and beta bands significantly correlates with higher executive performance.
Findings from our case study are consistent with those reported in a study on adults with Internet Gaming Disorder (IGD), where significantly elevated intrahemispheric fast-frequency coherence was identified as a potential neurophysiological trait marker of the disorder (Park et al., 2017; 2018). However, in contrast to our results, no significant EEG coherence changes were observed between pre- and post-treatment assessments in the IGD group across any frequency band.
This comparison underscores a key distinction: unlike conventional interventions in IGD populations, our multimodal therapeutic program—which included total screen detox and family-integrated neuroregulation—was able to produce measurable and clinically relevant changes in cortical connectivity within just five months. These results suggest that early-life screen-induced dysregulation may remain more neuroplastically responsive than similar conditions in adulthood, and that timely, intensive intervention can promote neural reorganization.
Conclusion
The hypothesis that therapy would be significantly more challenging in a 12-year-old child with a long-standing history of early-onset screen addiction and a diagnosis of atypical autism—compared to interventions in younger children aged 3 to 6—was partially confirmed.
Despite multiple severe withdrawal crises, regressions, and disruptions in sleep and behavior, the child demonstrated meaningful improvements across sensory, motor, affective, cognitive, and social domains. These changes were supported by quantitative EEG measurements showing significant reductions in cortical hypercoherence, particularly in the Beta 1, Beta 2, and Beta 3 frequency bands with eyes open, and in Beta 2 and Beta 3 bands with eyes closed.
The intervention also facilitated the normalization of previously elevated interhemispheric coherence, suggesting improved functional differentiation, hemispheric specialization, and maturation of cortical networks. These findings support the view that screen addiction in childhood induces neurophysiological patterns resembling those found in Internet Gaming Disorder (IGD), such as excessive fast-frequency coherence (Park et al., 2017; 2018). However, unlike in adult IGD interventions, our approach yielded measurable neurofunctional reorganization within a five-month period.
Nevertheless, the therapy did not lead to full recovery, nor to complete stabilization of sleep or emotional reactivity. Periods of regression continued to occur, particularly following suspected screen re-exposure and intensive therapeutic phases. Visual cortex coherence anomalies persisted, indicating that certain neural systems remained less responsive to the intervention within the observed timeframe. Additionally, the child remained vulnerable to environmental and relational stressors, and the therapeutic gains appeared fragile and dependent on caregiver consistency.
In sum, while the five-month intensive therapy led to neurophysiological and behavioral gains, it also revealed the limits of neuroplasticity in later developmental windows. These findings emphasize the urgency of earlier intervention, but also demonstrate that even at age 12, significant rewiring of cortical connectivity is possible—provided that treatment is immersive, sustained, and systemically supported.
References
Alexandrov, I.I, Manolova, V.R. and Vezenkov S.R. (2025) Infantile Behavior Patterns and Developmental Delays in Adolescents and Young Adults (Aged 12-29) with Screen Addiction. Nootism 1 (1), 79-82, ISSN 3033-1765 (print), ISSN 3033-1986 (online)
Basharpoor, S., Heidari, F., & Molavi, P. (2019). EEG coherence in theta, alpha, and beta bands in frontal regions and executive functions. Applied Neuropsychology: Adult, 1–8. doi:10.1080/23279095.2019.1632860
Manolova V.R. and Vezenkov S.R. (2025) Screen Trauma – Specifics of the Disorder and Therapy in Adults and Children. Nootism 1(1), 37-51, ISSN 3033-1765 (print), ISSN 3033-1986 (online) (1)
Manolova, V.R., Pashina, I.H., Mateev M.I, Vezenkov, S.R. (2025) Munchausen Syndrome by Proxy and Other Forms of Parental Abuse in Children with Screen Addiction and a Diagnosis of Autism (ASD) and/or ADHD. Nootism 1(2), 11-30, ISSN 3033-1765 (print), ISSN 3033-1986 (online) (2)
Pashina I.H., Manolova V.R. and Vezenkov S.R. (2025) Parental Recovery as a Key Factor for the Recovery of Children with Screen Addiction – Biofeedback Therapy for Severe Disorders. Nootism 1(1), 83-89, ISSN 3033-1765 (print), ISSN 3033-1986 (online)
Park, S. M., Lee, J. Y., Kim, Y. J., Lee, J. Y., Jung, H. Y., Sohn, B. K., Choi, J.-S. (2017). Neural connectivity in internet gaming disorder and alcohol use disorder: A resting state EEG coherence study. Scientific Reports, 7(1), 1333. https://doi.org/10.1038/ s41598-017-01419-7.
Park, S., Ryu, H., Lee, J. Y., Choi, A., Kim, D. J., Kim, S. N., & Choi, J. S. (2018). Longitudinal changes in neural connectivity in patients with internet gaming disorder: A resting-state EEG coherence study. Frontiers in Psychiatry, 9, 252. https://doi. org/10.3389/fpsyt.2018.00252.
Petkova, S. P., Manolova, V. R., & Vezenkov, S. R. (2025). Restoring attachment in children with early screen addiction. Nootism, 1(1), 74-78, ISSN 3033-1765 (print), ISSN 3033-1986 (online)
Petrov P.P., Manolova V.R. and Vezenkov S.R. (2025) Hidden Family Dynamics in a Case Study of a Child with Screen Addiction, Hyperactivity, and Language Deficits. Nootism 1(1), 90-95, ISSN 3033-1765 (print), ISSN 3033-1986 (online)
Petrova, S.N., Manolova V.R. and Vezenkov, S.R. (2025) Reintroducing Screens: Severe Regression and Symptom Aggravation in Children with ASD/Screen Addiction. Nootism 1(1), 59-65, ISSN 3033-1765 (print), ISSN 3033-1986 (online)
Sauseng P., Griesmayr B., Freunberger R., Klimesch W. (2010). Control mechanisms in working memory: A possible function of EEG theta oscillations. Neuroscience & Biobehavioral Reviews, 34, 1015–1022.
Sauseng, P., Klimesch, W., Schabus, M., & Doppelmayr, M. (2005). Fronto-parietal EEG coherence in theta and upper alpha reflect central executive functions of working memory. International journal of Psychophysiology, 57(2), 97-103.
Stefanova M.Ts., Manolova, V.R. and Vezenkov S.R. (2025) ADHD and Screen Addiction in Children Aged 3-9: Staged Recovery and Neurophysiological Markers. Nootism 1(1), 66-73, ISSN 3033-1765 (print), ISSN 3033-1986 (online)
Vezenkov, S. R., & Manolova, V. R. (2024). A Central Role of Biofeedback in a Complex Therapy of Screen Devices Usage Addiction. BFE 21tst Meeting Montesilvano, Italy, 21-22 September 2022, In APPLIED PSYCHOPHYSIOLOGY AND BIOFEEDBACK. Vol. 49, No. 1, pp. 173-173, https://doi.org/10.1007/s10484-023-09607-0 (1)
Vezenkov, S.R., Manolova, V.R. (2024) Rethinking Autism: The Screen Addiction Paradigm. BFE 22nd Meeting, 8-13 April 2024, Ljubljana, Slovenia, DOI: 10.13140/RG.2.2.27970.80328 (2)
Vezenkov, S.R., Manolova, V.R. (2025) Screen Addiction – Biomarkers, Developmental Damage and Recovery. Nootism 1(1), 6-18, ISSN 3033-1765 (print), ISSN 3033-1986 (online) (1)
Vezenkov, S.R. and Manolova V.R. (2025) Neurobiology of Autism/Early Screen Addiction Recovery. Nootism 1(1), 19-36, ISSN 3033-1765 (print), ISSN 3033-1986 (online) (2)
Vezenkov, S.R., Manolova, V.R. (2025) Screen-Induced Pathological Vestibular Reflex: A Specific Marker of Early Screen Addiction. Nootism 1(2), 5-10, ISSN 3033-1765 (print), ISSN 3033-1986 (online) (3)