

Stoyan R. Vezenkov and Violeta R. Manolova
Center for applied neuroscience Vezenkov, BG-1583 Sofia, e-mail: info@vezenkov.com
For citation: Vezenkov S.R. and V.R. Manolova (2026) Screen Addiction in Children and Adults: Biomarkers, Screen Trauma and Reversed Development. Nootism 2(1), 4-45, https://doi.org/10.64441/nootism.2.1.1

This report was presented at the BFE 24th meeting on 25 March 2026 in Poland. An incomplete version of the report was first presented at the NRBS Conference on 25 October 2025 in New York.
Abstract
This report presents a comprehensive synthesis of hundreds of clinical cases involving adults and children diagnosed with screen addiction (TV, internet, gaming, social media, pornography, shopping etc.), integrating proprietary innovations derived from instrumental research (qEEG, ANS) and complex therapy including biofeedback. As its prevalence rises, observed symptoms frequently mimic or overlap with established diagnoses such as Autism Spectrum Disorder (ASD), ADHD, Oppositional Defiant Disorder (ODD), OCD, PTSD, depression, anxiety, various personality disorders, tics, occipital and other forms of epilepsy and many others.
Despite the emergence of awareness campaigns, the prevailing discourse continues to frame the issue merely as 'screen time' or 'digital media use.' This terminology obscures the essential reality: we are confronting a severe addiction that systematically disrupts regulatory mechanisms, leading to profound clinical symptoms and developmental disturbances. Regrettably, this pathology is frequently underestimated by the broader therapeutic community, and Biofeedback practitioners are no exception.
The report introduces a holistic conceptual framework for understanding this pathology, proposing new terminologies and revising existing constructs to facilitate the establishment of effective therapeutic approaches. Key contributions include:
- Biomarkers & Mechanisms: Identification of neurobiological mechanisms and specific biomarkers for screen addiction, including early-onset cases.
- Screen Trauma: Definition of "Screen Trauma," including its formation and the persistence of cue-dependent behaviors.
- Screen-induced Pathological Reflexes: Screen-Induced Pathological Vestibular Reflex (SIPVR) and Screen-Induced Pathological Eye Covering Reflex (SIPECR), alongside absent or impaired nystagmus, screen-induced synesthesia, cue-dependent behaviors, and repetitive motor stereotypies such as toe walking and hand flapping.
- Developmental Regressions: Description of developmental anchors, cortical fragmentation and splitting or "reversed development" (regression toward intrauterine or animalistic behavioral models) as a maladaptive coping strategy for maintaining trauma-addiction primitive biopsychosocial homeostasis.
- Learning Deficits and Shifts: Analysis of hypermnesia, Gaming Transfer Phenomena (GTP), sensory fragmentation (both hyper- and hypo- sensitivity) and poor executive skills, and compromised attentional, memory and learning systems (associative, instrumental, and mirror).
- Language Impairments: Manifesting as absent or impoverished speech (e.g., echolalia), or as a distinct regression in language skills.
- Identity and Self-Processing Deficits: Characterized by an undeveloped sense of Self and awareness of Others (clinically observed as a lack of eye contact). Aberrant functional connectivity between the Default Mode Network (DMN) and the Executive System, mediated by inverted Salience Network modulation. Clinical symptoms include dissociation, depersonalization, and the construction of a pathological "Virtual Self."
Furthermore, the report proposes a new framework for the interaction of regulatory systems across sleep-wake cycles, addressing the inversion of internal/external processing, fragmentation, splitting, and psychotic-like states.
It critically challenges the validity of ASD diagnoses and presumed neurodivergent functioning, demonstrating that these symptoms remit following the treatment of screen addiction, the resolution of associated screen trauma, and the patient's return to human reality. It highlights strategies for providing effective screen and digital detox, emphasizing that the re-introduction of screens consistently precipitates a potent behavioral regression and symptom recurrence.
The core principles of the proposed complex therapy for screen addiction include:
- Total screen/digital detox.
- Contain and neutralize "animalistic programs for control and dominance" (evolutionarily conserved defensive circuits).
- Master tantrums and hysterical episodes.
- Sequentially lift developmental anchors (SIPVR, SIPECR, lack of nystagmus), dissolving induced synesthesias and cue-dependent behaviors.
- Awaken the cortex via sensory “Restart” and contextualized behavior.
- Reconnect the child with the therapist and parent.
- Develop language within a social context.
- Parallel therapy and parental education, preparing parents to re-attach and become guides, not "service staff."
- Prevention guidelines: digital hygiene and prevention strategies for both healthy individuals and patients in post-therapy maintenance.
The report elucidates the concept of Nootism as a practice-derived framework designed to restore children and adults from screen addiction and associated trauma to human connectedness and typical development.
Keywords: Screen Addiction, Screen Trauma, Biomarkers, Reversed Development, Digital Detox, Nootism, Neurodevelopmental Regression, Screen-Induced Pathological Reflexes (SIPVR, SIPECR), Cue-Dependent Behavior, Autism Spectrum Disorder (ASD), qEEG, HRV, biofeedback
Learning objectives:
- Differentiate the clinical presentation of Screen Addiction from overlapping neurodevelopmental diagnoses (such as ASD, ADHD, and ODD) by recognizing specific neurobiological biomarkers and observing symptom remission following complex therapy.
- Identify the physiological signs of "Screen Trauma," including unique Screen-Induced Pathological Reflexes (SIPVR, SIPECR), impaired nystagmus, and the development of cue-dependent behaviors and motor stereotypies.
- Explain the underlying neurophysiological mechanisms of screen addiction, specifically the "inverted" modulation of the Salience Network and the aberrant coupling between the Default Mode Network (DMN) and the Executive System.
- Apply the core therapeutic principles of "Nootism" – ranging from total digital detox and the neutralization of primitive defensive circuits to the re-establishment of parental authority – to restore human connectedness.
This article synthesizes a conceptual framework developed over the last decade through clinical work with children, adolescents, and adults. This work has increasingly suggested that screen addiction should be approached not merely as excessive media use, but as a serious biopsychosocial disorder with neurodevelopmental, autonomic, behavioral, and relational consequences. In the youngest children, these consequences may be especially profound. The conceptual framework presented here emerged from therapeutic work at the Center for Applied Neuroscience Vezenkov and was articulated across two plenary conference presentations: The Developing Brain and Early Screen Addiction: Uncovering the Hidden Neurobiology of Autism and ADHD, delivered in Manhattan, New York, on 25 October 2025 at the NRBS Annual Conference, and Screen Addiction in Children and Adults: Biomarkers, Screen Trauma and Reversed Development, delivered at the 24th Meeting of the Biofeedback Federation of Europe in Szczecin, Poland, on 25 March 2026.
Short introduction
The world is changing faster than families, clinics, and schools can absorb. Relationships are eroding, parents increasingly feel under siege, and the development of children appears to be moving in a direction for which few clinicians, educators, or caregivers were adequately prepared. Within this broader crisis, one of the most underestimated forces may be screen addiction and, increasingly, dependence on AI-based toys, robots, and digital companions. The central question is no longer whether technology is useful, but where use ends and addiction begins, and what that addiction does to human development, freedom, identity, and relational life.
Our hope is that, by understanding the mechanisms of addiction and identifying paths to treatment and recovery, we can still help children, families, and adults reclaim what is human while living in a digital world.
First, however, we must recognize the addiction that is reshaping mind, body, and relationships.
The present article’s purpose is not to offer a finalized causal model, but to formulate a clinically grounded and testable conceptual framework. The framework proposes that severe screen addiction, especially in early development, may alter attention, mirroring, attachment, reward processing, autonomic regulation, sensory integration, and language development in ways that produce clinical pictures of autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD), oppositional defiant disorder (ODD), and related neurodevelopmental presentations. (Stefanova et al., 2025; Vezenkov & Manolova, 2024, 2025c, 2025b)
At the center of this model stand several interlocking concepts: screen addiction, screen trauma, developmental anchors, cortical fragmentation, and reversed development. Together, these concepts are used to explain why some children do not simply show developmental delay, but rather enter a pathological homeostasis organized around sensory dominance, compulsive regulation, and retreat from human reciprocity. The article also outlines Nootism, a practice-derived therapeutic framework aimed at restoring wakefulness, attachment, language, and human connectedness after screen-mediated developmental dysregulation.
Personal Motivation and Ethical Frame
The Vezenkov Center for Applied Neuroscience, based in Sofia, Bulgaria, and since last year also in Weinheim, Germany, works primarily with biofeedback, EEG neurofeedback, in the treatment of psychosomatic disorders, irritable bowel syndrome (IBS), insomnia, pain, anxiety, depression, stress management, addictions and neuro-trainings for peak performance. (Vezenkov, 2016, 2023; Vezenkov & Iliev, 2019; Vezenkov & Manolova, 2025a; Vezenkov & Mitev, 2015) Our work with adolescents and adults led us to define and treat screen addiction in its many forms - gaming, social media, pornography, gambling, compulsive online use, and related patterns. Families of children diagnosed with ASD or ADHD repeatedly described strikingly similar developmental histories: very early and prolonged screen exposure, impaired language development, reduced eye contact, severe dysregulation when screens were removed, and behavioral dependence on audiovisual stimulation. (Alexandrov et al., 2025, 2025; Pashina et al., 2025; Petrov et al., 2025)
This convergence forced a clinical question: could a substantial subgroup of young children presenting with ASD-like or ADHD-like symptoms be suffering not only from developmental vulnerability, but from severe early screen addiction and its sequelae? This question led to direct therapeutic work with the youngest children and their families and eventually to the emergence of Nootism as a broader therapeutic and conceptual framework. (Ivanova et al., 2025; Manolova et al., 2025; Manolova & Vezenkov, 2025e; Petrova et al., 2025; Stefanova et al., 2025; Vezenkov & Manolova, 2025b)
The ethical motivation of this work is equally important. The model does not seek to stigmatize parents, deny biology, or reduce all developmental issues to screen exposure. Rather, it argues that if even a subgroup of children are being misclassified while suffering from a partly environmentally induced and potentially reversible condition, then clinicians and researchers are obliged to differentiate phenotypes more carefully, modify developmental environments, and assess therapeutic outcomes systematically.
Screen addiction (Roadmap)
We begin with the neurobiological mechanisms: how repetitive audiovisual stimulation may “hack” the mirror neuron system, the reward circuitry, and the polyvagal pathways. In this framework, the screen is not treated as a neutral medium, but as an active regulator of attention, arousal, and learning.
We then turn to the clinical picture - what “reversed development” means and how it may manifest in hyperactivity, language collapse, sensory fragmentation, and dysregulated behavior. These manifestations often resemble established neurodevelopmental diagnoses, which makes differential interpretation especially difficult.
We also examine why early screen exposure may function as a powerful epigenetic factor, reshaping the brain’s developmental trajectory before self-regulation has fully emerged.
Let me state the thesis clearly: the effectiveness of any therapeutic approach - medical, psychological, neurotherapeutic, biofeedback, or neurofeedback - declines sharply when screen addiction is not identified and addressed. In our time, screen-mediated dysregulation is no longer a marginal phenomenon; it is increasingly becoming part of the clinical background of nearly every person and family.
For this reason, I believe that no serious therapeutic model today can afford to ignore the role of screen addiction.
This leads to a deeper question: how does screen stimulation act upon the human brain - nature’s most extraordinary creation, shaped for creativity and open-ended development - and transform it into a rigid, stereotyped, and change-resistant system that defends its own status quo with remarkable intensity? This question is central to both clinical practice and developmental theory.
Let us begin with the youngest children. In our clinical experience, a substantial subgroup of children in the 3–6-year age range, labeled as ASD-, ADHD-, ODD-, or PDD-like and presenting with severe language deficits, also show a highly consistent profile of severe early screen addiction, screen trauma, or what we call reversed development.
This is not a dogma, but a clinical hypothesis derived from repeated observations, recurring developmental histories, and consistent changes following therapy. It should be challenged - as any serious hypothesis should be. My aim is to offer an explanatory framework that is both clinically useful and open to empirical testing.
Severe early screen addiction is not defined simply by high screen time. Rather, it is characterized by compulsive seeking of high-intensity, low-social-density sensory stimulation; cycles of soothing followed by dysregulation; a shift of interest away from human faces and toward objects, colors, shapes, and repetitive sensory patterns; and a collapse of joint attention and eye-to-eye interaction.
Screen trauma refers to the durable imprinting of these patterns, such that even after the removal of devices, the child remains anchored in infantile, sensory-dominant, and dysregulated modes of functioning.
Developmental anchors are the screen-induced pathological reflexes, sensory distortions, cue-dependent behaviors, and regulatory loops that continue to pull the child backward under stress, change, or overload. These anchors help explain why detox alone is often insufficient.
A further extension of this thesis is the concept of reversed development. This term describes a pathological reorganization in which older, evolutionarily more primitive survival systems begin to dominate higher human systems of reciprocity, language, and self-regulation.
Within this framework, the problem is not only developmental arrest, but a deviation toward a narrower and qualitatively different mode of psychophysiological organization. In this sense, the child is not merely delayed, but reorganized around survival rather than development.
The Developing Brain 0–9 Years: Sensitive Windows
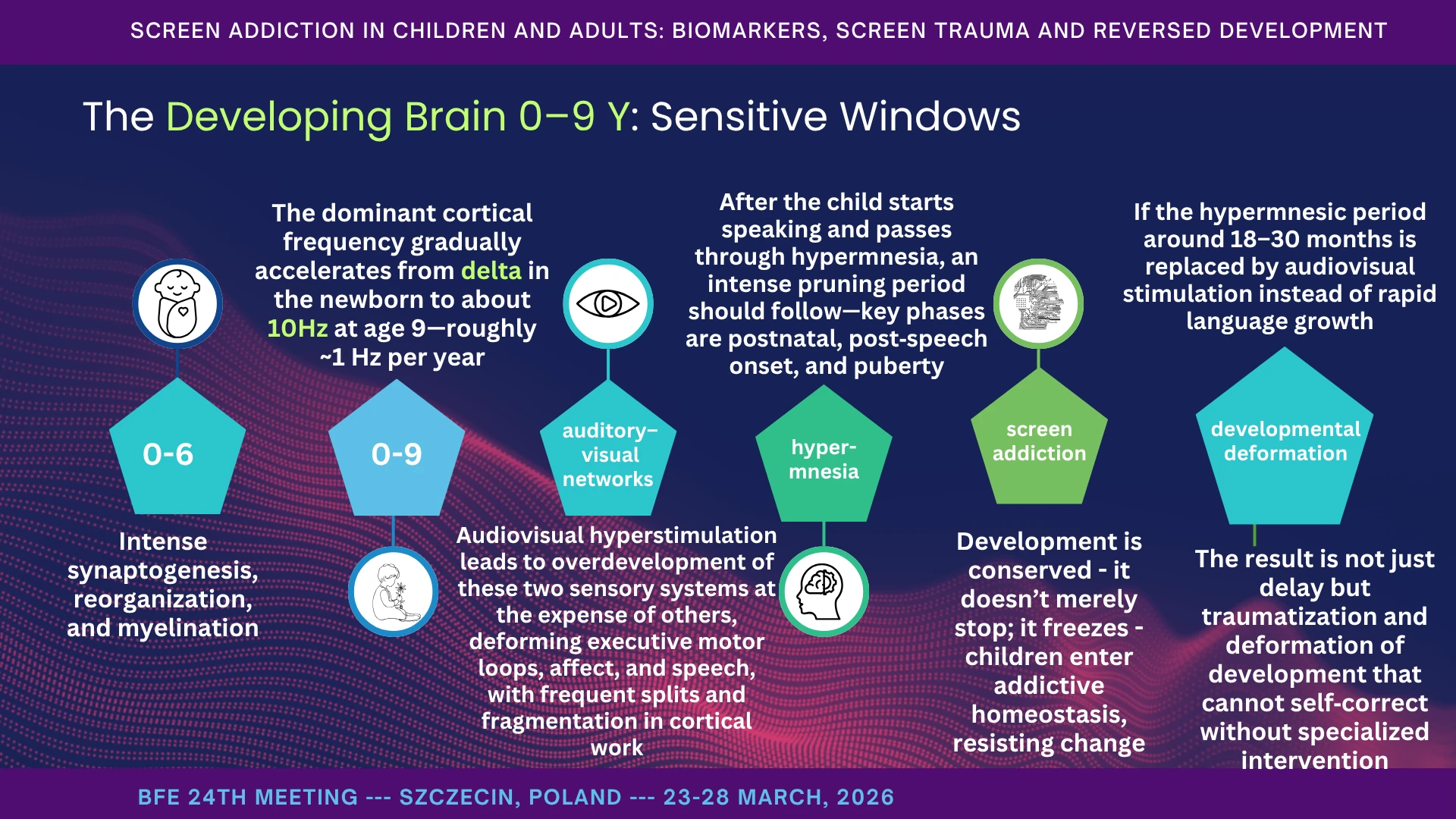
The developing brain does not simply grow; it calibrates itself to the environment. The first six years of life - up to the shedding of the primary teeth - constitute a period of intense synaptogenesis, reorganization, and myelination, during which the brain is effectively deciding what matters: which sounds are meaningful, which faces are important, which rhythms signal safety, and how the child learns to self-soothe and regulate (Vezenkov & Manolova, 2025c, 2025b)
Myelination is a staged and experience-sensitive developmental process that contributes to brain function and plasticity across early life. (de Faria et al., 2021)
In a human environment rich in movement, touch, rhythm, eye contact, and language, the brain prunes excess connections and strengthens those that support attention, language, and self-regulation. When, however, the environment is dominated by fast, repetitive audiovisual stimulation, the brain strengthens those pathways instead. In this sense, screens do not simply distract development; they actively train it.
Early childhood includes sensitive periods during which experience is uniquely influential in shaping neural circuitry and later developmental outcomes. (Zeanah et al., 2011)
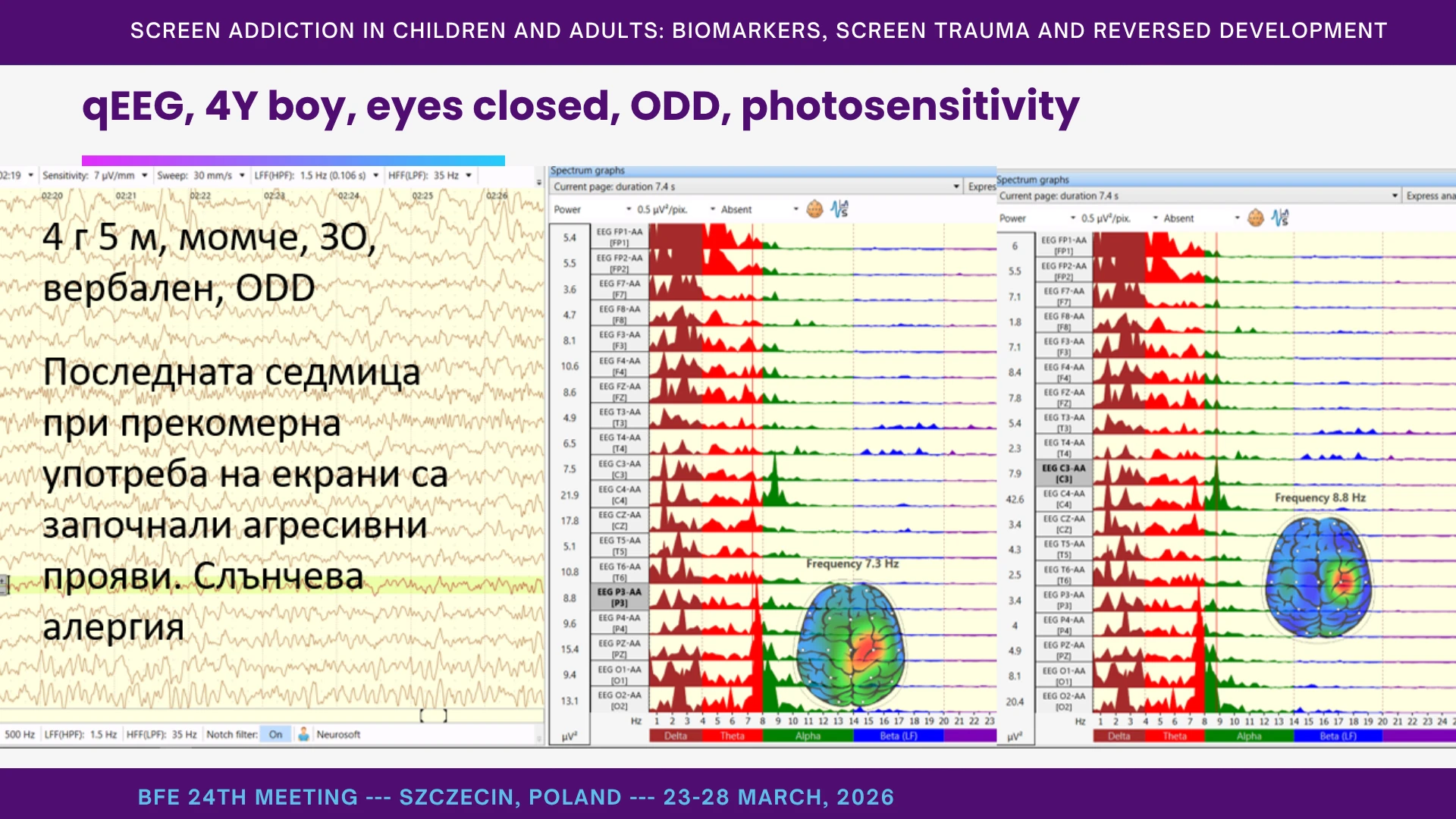
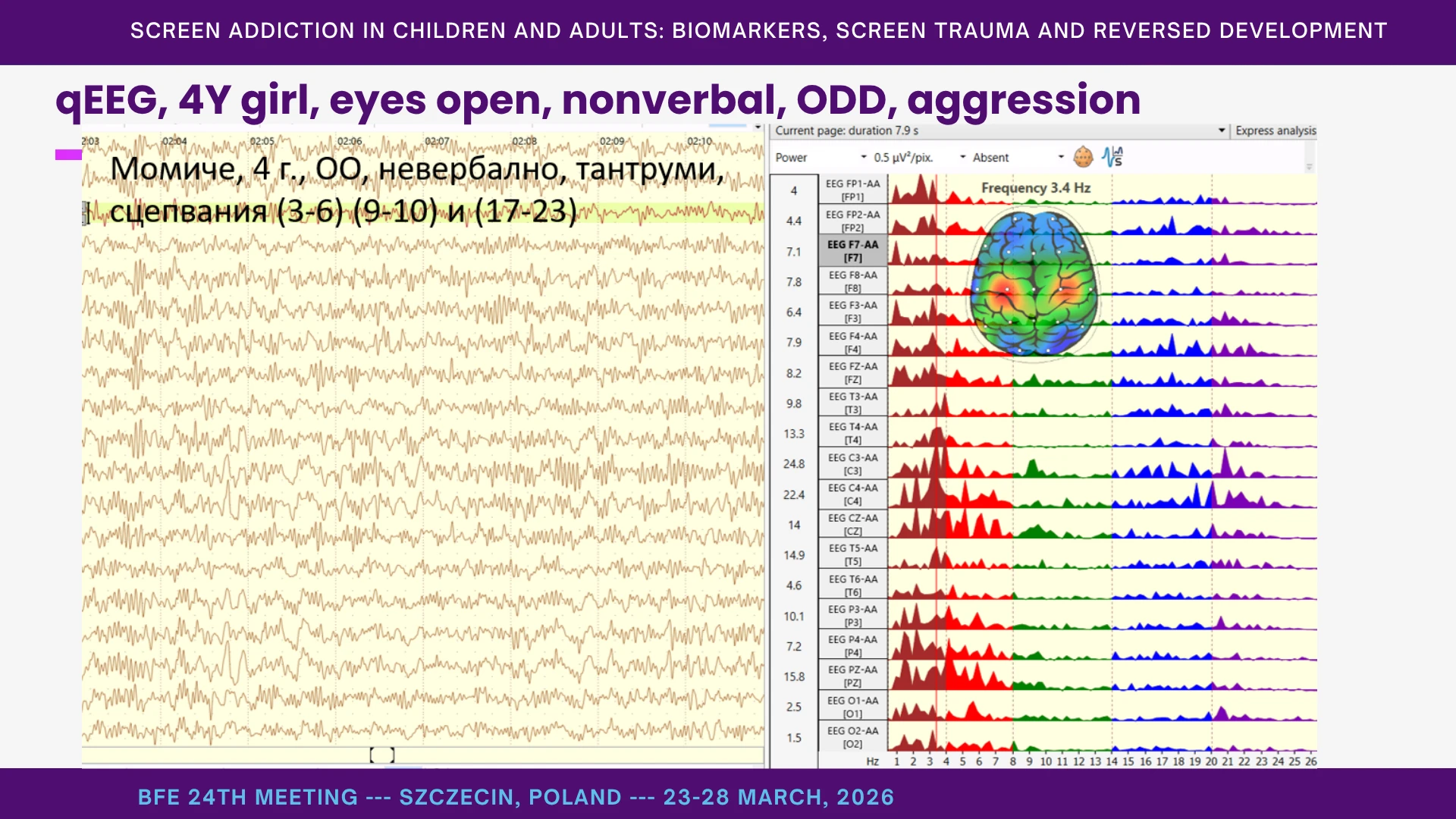
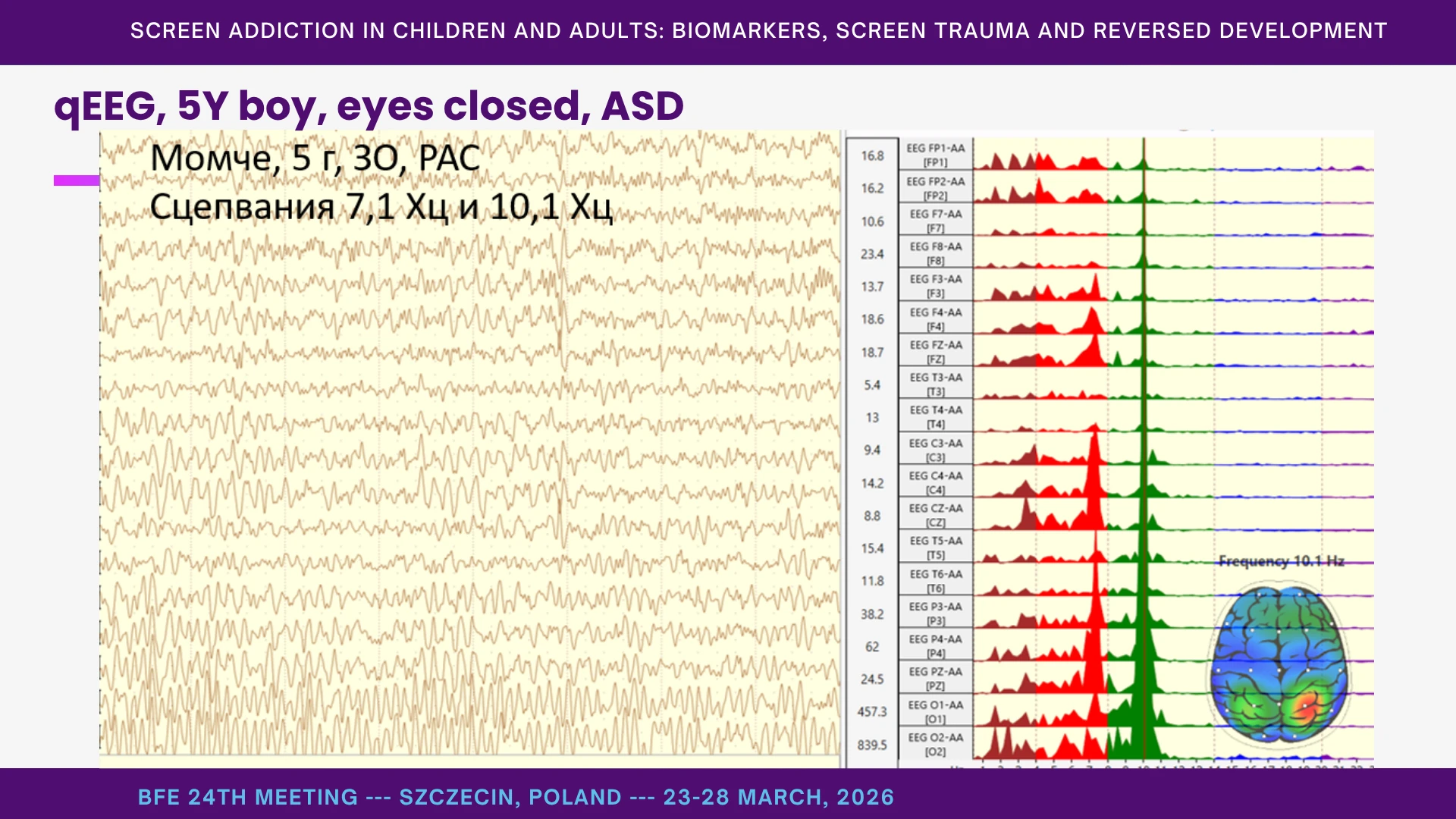
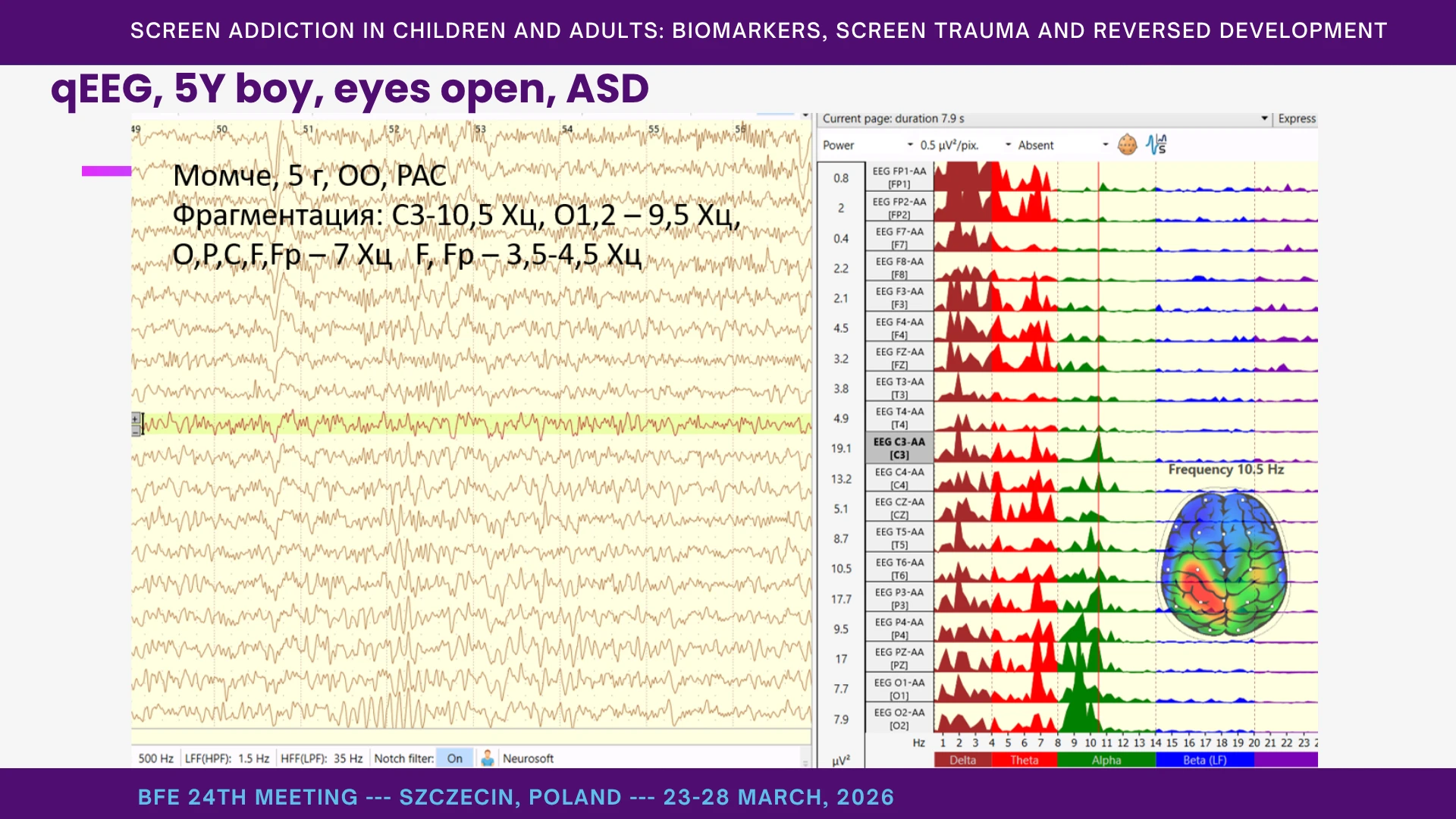
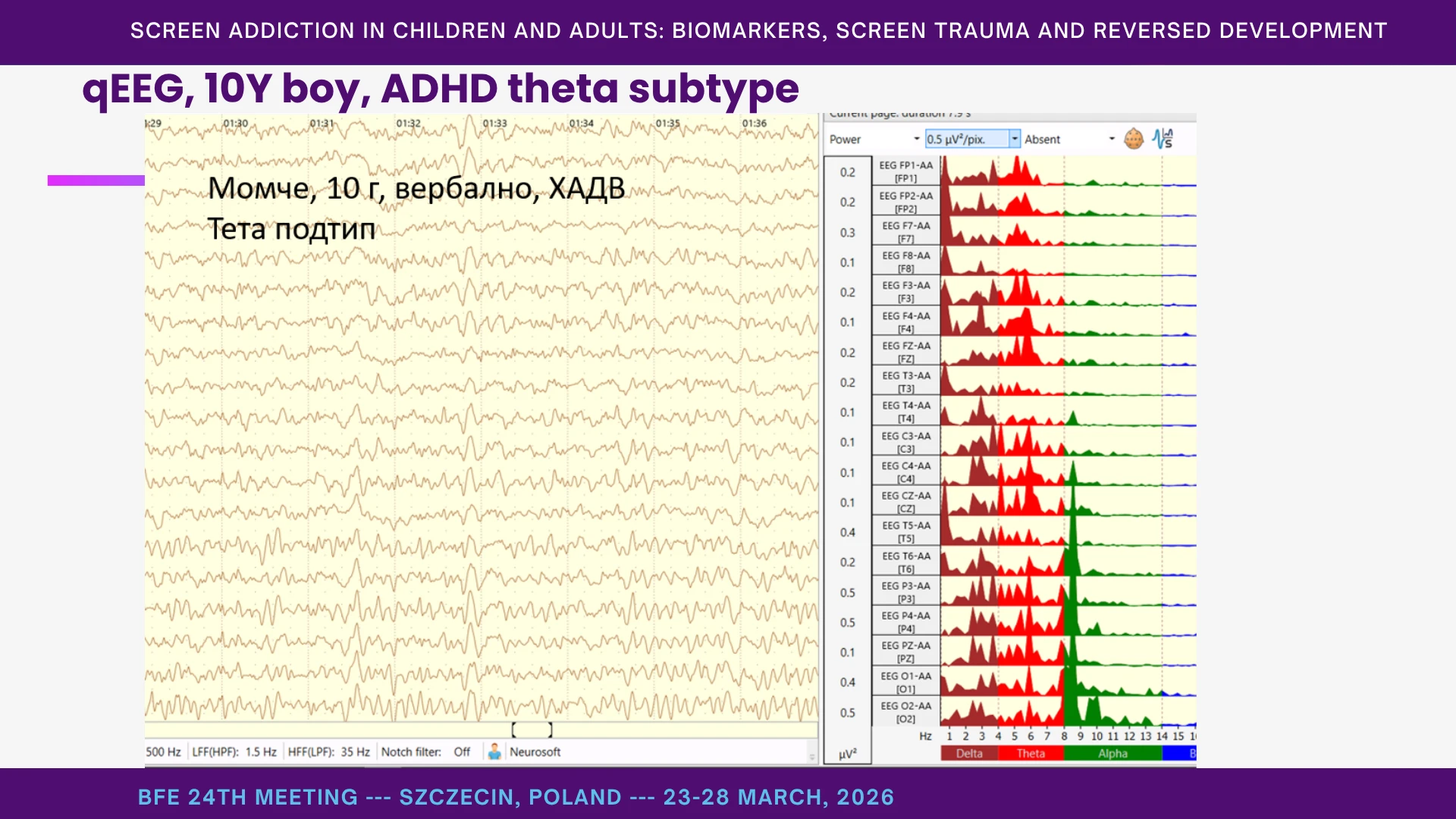
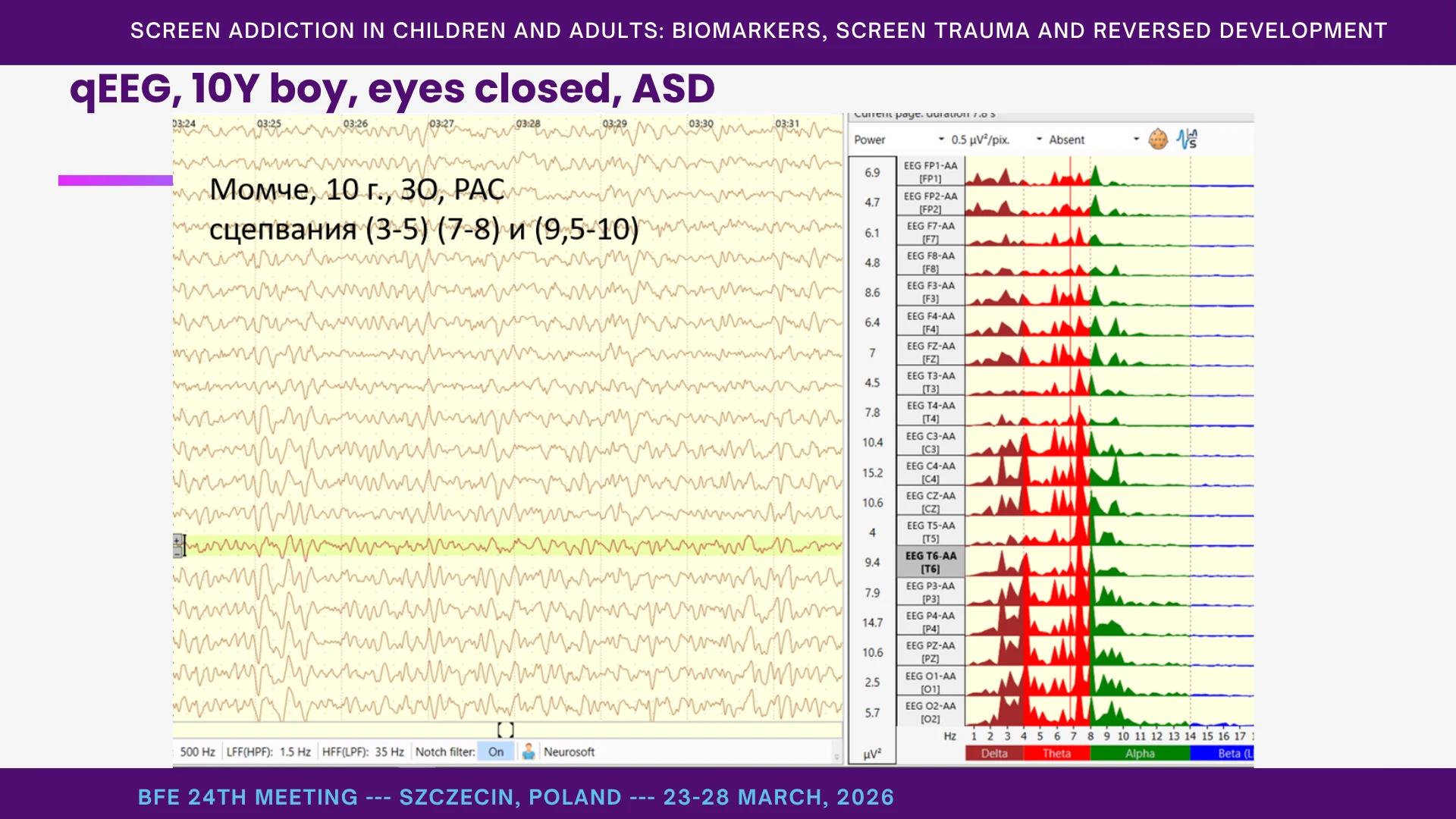
We also observe in clinical practice that highly salient developmental experiences - or, conversely, traumatic and addictive ones - may leave age-linked signatures in dominant cortical rhythms. For example, when screen addiction begins before 18 months, dominant peaks are often observed at 2–3 Hz; between 18 and 30 months, at 3–4 Hz; and between 30 and 36 months, at 4–5 Hz. This should be presented as a practice-derived hypothesis rather than an established developmental rule, but it has repeatedly corresponded to parental histories of early screen exposure in our clinical material (Stefanova et al., 2025; Vezenkov & Manolova, 2025b).
Audiovisual hyperstimulation appears to promote overdevelopment of visual and auditory processing at the expense of other sensory and integrative systems, thereby deforming executive-motor loops, affect regulation, and speech development, with frequent splitting and fragmentation in cortical functioning. Clinically, this may present as a higher dominant frequency in posterior leads than in central and frontal regions, increased slow-wave amplitudes in the left hemisphere relative to the right, and multiple neural networks operating at distinct dominant frequencies without adequate integration. High-amplitude alpha activity in O1 has been repeatedly observed as a common biomarker of screen addiction, including in children (Vezenkov & Manolova, 2025c; Zlatkova, 2025).
Within this framework, auditory-visual networks become tuned to specific stimuli at the expense of social perception, while slow-wave frontal automatism begins to replace goal-directed behavior and executive functioning. Clinically, this may be reflected in cue-dependent behaviors such as defecation or feeding only in the presence of a specific color or shape, or calming only through particular spatial or color stimuli.
A second key process is pruning. Human cortical synaptogenesis peaks in infancy and is followed by progressive synapse elimination that is especially rapid during the preschool years, underscoring the plasticity and vulnerability of early development. (Huttenlocher, 1984) After early vocabulary growth and hypermnesia, development should normally proceed through phases of reorganization and selection. In severe screen addiction, this process often does not unfold typically. Development does not merely slow down; it becomes arrested around repetitive, high-reward patterns, and children enter a state of addictive homeostasis characterized by resistance to change.
In clinical practice, we encounter 12-year-olds who have still not shed their primary teeth, as well as children with delayed acquisition of bowel and bladder control. Slow-wave cortical activity is associated, in our model, with poor impulse control and the persistence of automatic sensorimotor programs reinforced by the law of effect. The assertion of the child’s will over caregivers is developmentally characteristic of ages 2 to 3, but here two parental patterns often diverge sharply: permissive parenting and neglectful or inadequate parenting. In the former, children become “emperors,” while adults begin to function as support staff for a narrow range of automatic programs, thereby amplifying the addiction loop; in the latter, the child may sink into a private world even in the absence of screens (Ivanova et al., 2025; Manolova et al., 2025; Mateev, Manolova, et al., 2025; Mateev, Pashina, et al., 2025; Pashina et al., 2025; Petrov et al., 2025; Petrova et al., 2025; Vezenkov & Manolova, 2025b).
As a result, the child may accumulate fragments - words, scripts, colors, routines, without developing an integrated language system or socially meaningful behavior. If the hypermnesic period around 18–36 months is replaced by audiovisual stimulation rather than rapid language growth, the result is not merely delay, but traumatization and deformation of development that may not self-correct without specialized intervention. Recent meta-analytic evidence suggests that screen-use context matters: more program viewing and background television are associated with poorer cognitive outcomes, while caregiver co-use is associated with better cognitive outcomes. (Mallawaarachchi et al., 2024)
This is why a child may produce many words, even in several languages, and still not possess language in the true developmental sense. Language is not the mere production of words; it is the use of words within shared human context, reciprocity, and meaning.
In preschool-aged children, greater screen-based media use has been associated with lower microstructural organization and myelination of white-matter tracts that support language and emergent literacy. (Hutton et al., 2020) Systematic-review evidence indicates that greater screen use is associated with poorer language outcomes in early childhood. (Hutton et al., 2020) Longitudinal evidence from infancy to 5 years shows a predictive negative association between children’s screen media exposure and vocabulary development. (Sundqvist et al., 2024) Higher screen time between 12 and 36 months has been associated with fewer adult words, fewer child vocalizations, and fewer conversational turns, suggesting that screen exposure may displace language-rich interaction. (Brushe et al., 2024)
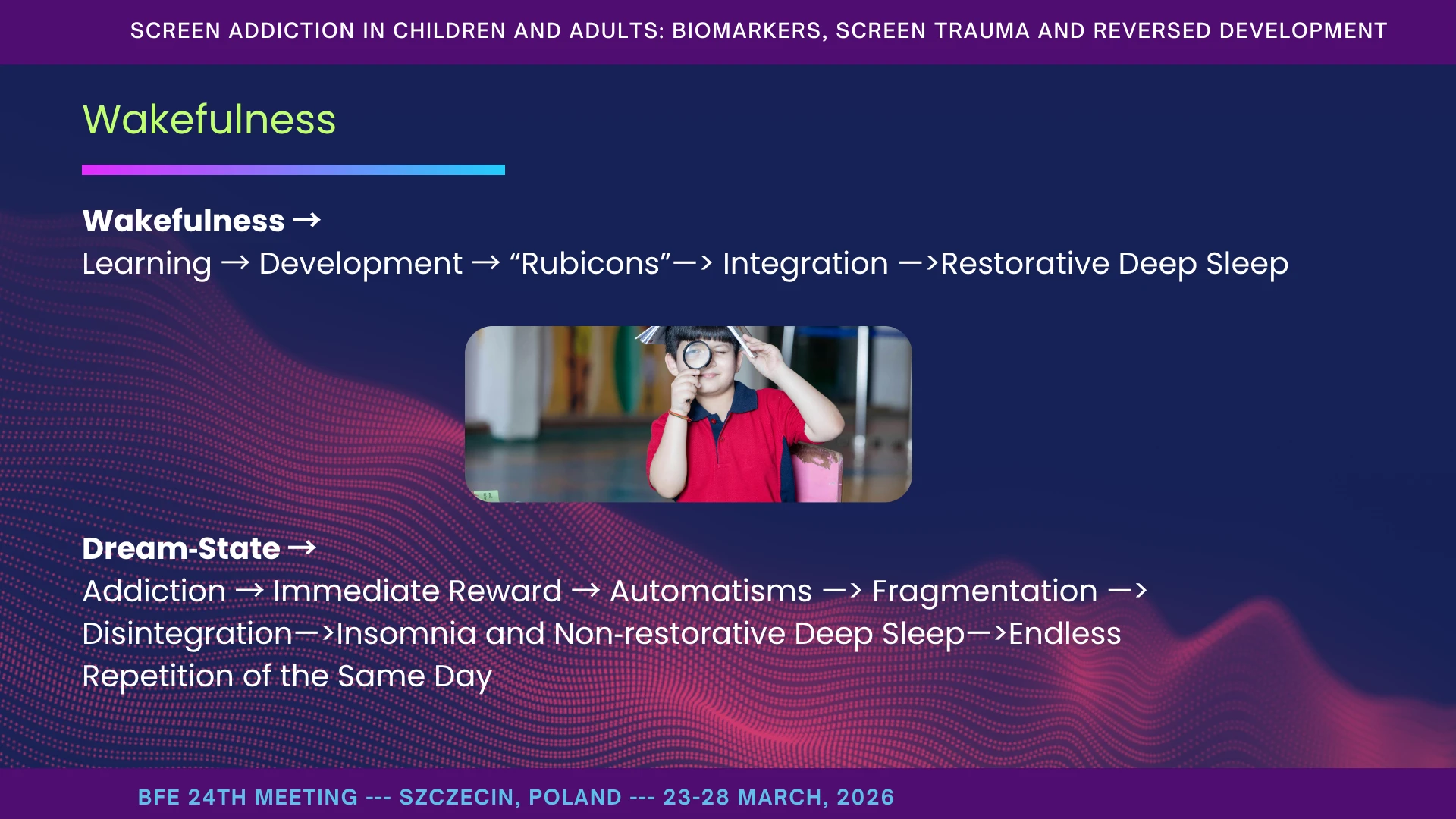
Wakefulness
Wakefulness is not merely being awake. It is cortical readiness for human connection: the child sees your face, hears your voice, feels rhythm, and is available for shared meaning (Birulés et al., 2023; Dresp-Langley, 2020a; Mercure et al., 2019; Mundy & Newell, 2007; Zhang et al., 2022). This is the “learn from people” mode, as opposed to being cut off in a world of compulsions and automatisms. Joint attention is reliably associated with both concurrent and later receptive and expressive language outcomes, highlighting the importance of socially shared attention for language development. (Bottema‐Beutel, 2016) This mechanism is fundamental for language acquisition and social competence, as it activates distributed cortical networks that integrate self-intentions with the goal-related behaviors of others. Infants show phonetic learning from live social exposure, but not from prerecorded audiovisual or audio-only exposure, suggesting that early language learning is strongly facilitated by social interaction rather than passive perceptual input alone. (Kuhl et al., 2003) In infancy, attention to face-to-face social interaction predicts later phonetic learning, supporting the view that early language acquisition depends on socially engaged, contingent interaction. (Conboy et al., 2015)
At the opposite pole is dream-state: a mode of automatisms, immediate reward, and repetitive sensory capture. In itself, this mode is not pathological; all of us use it for habit and routine. The problem arises when it becomes dominant in a young child. Screens pull children into dream-state with extraordinary ease: fast rhythm, high contrast, predictable cuts, instant reward. The child does not need to wait, track a face, tolerate ambiguity, or work for meaning; everything arrives ready-made, without effort.
From there, a sensory addiction loop begins to form: stimulation, soothing, then more stimulation. With repetition, tolerance for boredom, waiting, and human pacing decreases. Automatisms consolidate. We begin to see rituals in which a screen is required for feeding, sleeping, dressing, or calming. Remove it and observe withdrawal: crying, hysteria, aggression - not because the child is “bad,” but because we cut their regulatory prosthesis.
Higher screen time between 12 and 36 months is associated with fewer adult words, fewer child vocalizations, and fewer conversational turns, suggesting that screen exposure may displace the language-rich interactions on which early development depends. (Brushe et al., 2024)
In this mode, the brain can learn without integration. Sounds and images are stored, but detached from human context. That is why we see islands of knowledge: a child can count to twenty with a song, recite multiple alphabets by rote, or reproduce astonishing fragments from clips and advertisements, yet still fail to understand a simple human request such as “give me two apples.” This is not a deficit of attention or intellect; it is a deficit of human meaning and social integration. (Madigan et al., 2019)
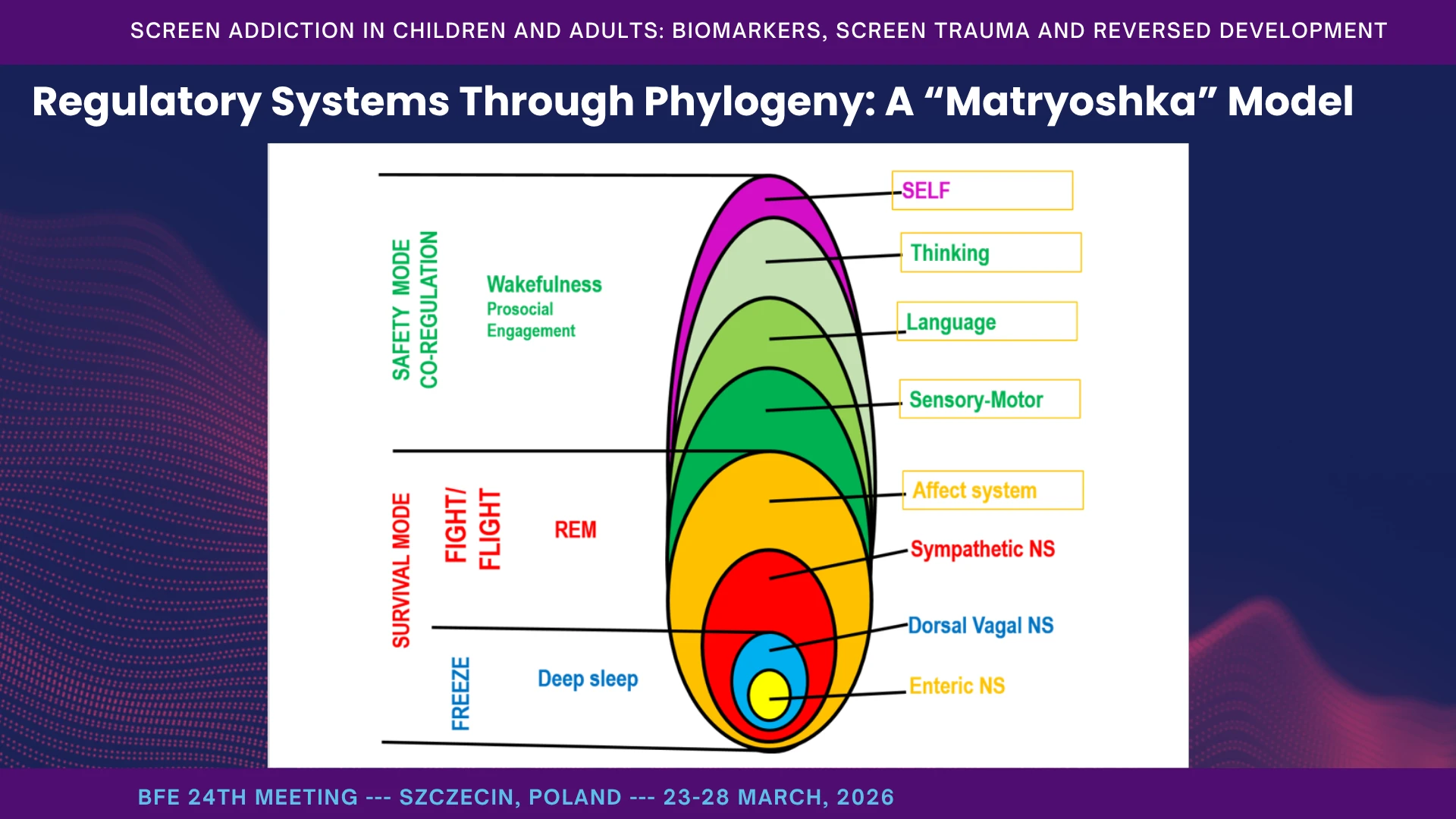
Regulatory Systems Through Phylogeny: A “Matryoshka” Model
I think of regulation as a set of nested matryoshka dolls. At the innermost level is diffuse, enteral regulation - the kind of basic physiological organization we see in very simple life forms. Above that is slow parasympathetic regulation, supporting deep sleep, conservation, growth, oxygenation, and passive survival. Above that come active survival systems - mobilization, fight, flight, and defensive action - shared across increasingly complex animal forms. Higher still are mammalian social systems, including the ventral vagal complex, where regulation becomes relational: face, voice, touch, rhythm, play. And above these stand the higher cortical systems - affect regulation, sensorimotor control, language, cognition, and the self-actualizing self-linked to wakefulness, planning, monitoring, and self-regulation. The image of nested dolls perfectly illustrates a core neurobiological principle first proposed by neurologist John Hughlings Jackson: dissolution. Jackson postulated that higher (phylogenetically newer) neural circuits naturally inhibit lower (older) ones. (Jackson, 1884)
Why the matryoshka image? Because in sleep, in shock, and under overwhelming stress, the higher layers can give way, and control passes downward to older systems. That is adaptive in the short term. But when this happens repeatedly in early childhood, it can become a developmental trajectory. Hyperstimulation without human content, together with chronic use of the screen as a soother, can hold the child in the inner dolls - in automatisms and reflexive regulation instead of social engagement and language.
I do not present this as dogma, but as a useful map. It helps explain why, in some children, we see evolutionarily older survival reactions - freezing, spinning, fleeing - where we would expect social reciprocity, flexible attention, and language. Our therapeutic task is to help the child build each regulatory layer so that every level can self-regulate without immediately handing control downward under minimal stress or environmental change. In the next slides, I will make this more concrete through the polyvagal framework. From a phylogenetic perspective, defensive responses such as fight, flight, and freeze, and social engagement behaviors are organized in a hierarchical neural architecture that supports adaptive regulation across contexts. (Porges, 2003) Polyvagal theory proposes that autonomic regulation is phylogenetically organized, with distinct neural circuits supporting immobilization, mobilization, and social communication. (Porges, 2009) Recent formulations of polyvagal theory emphasize the evolutionary transition from defensive autonomic states toward sociality, highlighting safety and co-regulation as central to adaptive functioning. (Porges, 2021) Coregulation involves mutual adaptation between partners at biological and behavioral levels and plays a crucial role in the development of self-regulation. (Bornstein & Esposito, 2023)
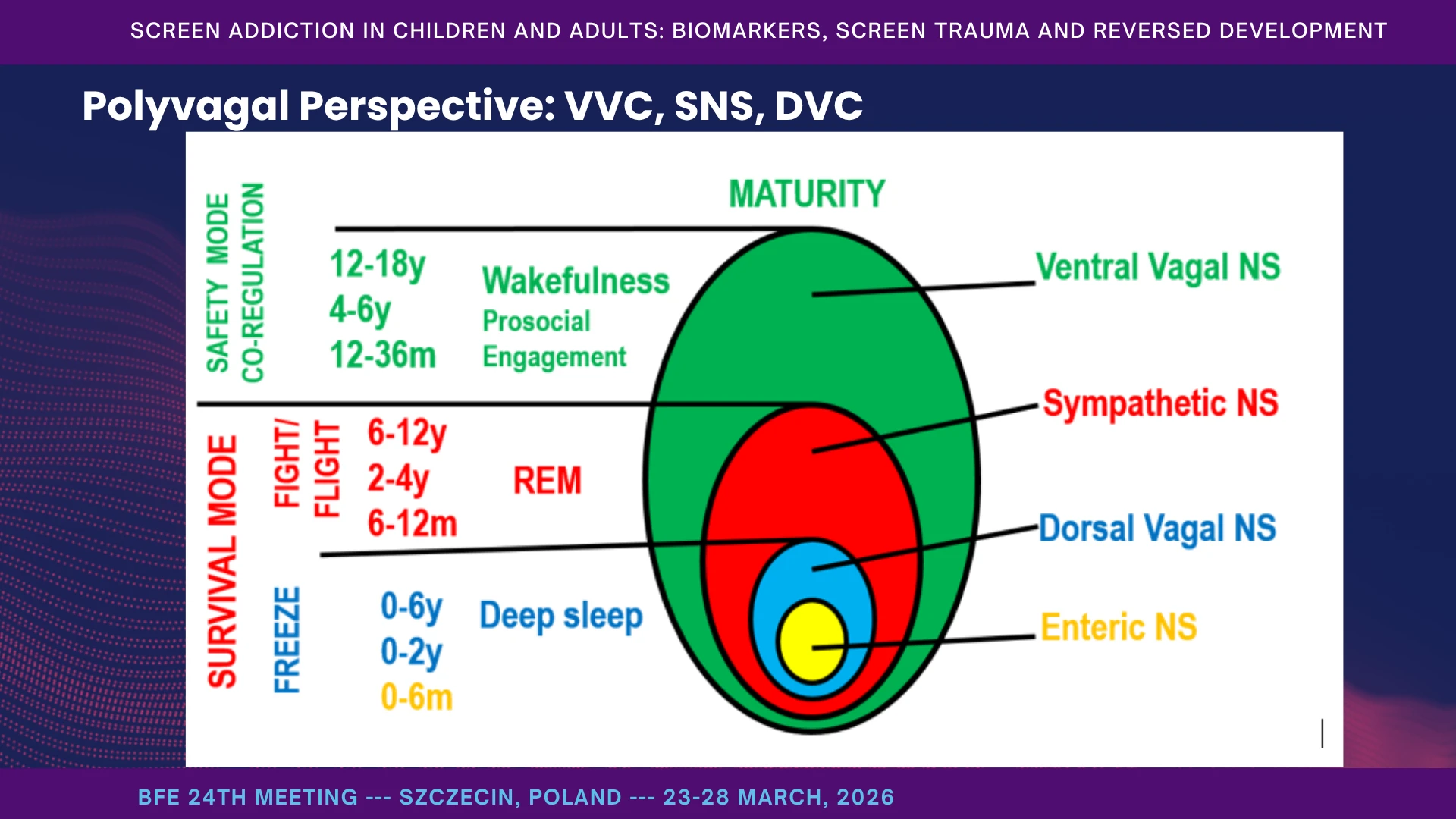
Polyvagal Perspective: VVC, SNS, DVC
The polyvagal framework helps us think in terms of three dominant regulatory states. The ventral vagal complex, or VVC, is the state of social engagement: soft gaze, warm prosody, flexible attention, play, and connection. The sympathetic nervous system, or SNS, is mobilization: fight, flight, rapid pulse, readiness for action. The dorsal vagal complex, or DVC, is immobilization: freeze, shutdown, low energy, and withdrawal. With safety and human connection, VVC tends to dominate; with threat or hyperstimulation, SNS takes over; with hopelessness or overwhelming overload, the system drops into DVC.
Recent summaries of polyvagal theory continue to emphasize the hierarchical autonomic model, the ventral vagal complex in social behavior, and neuroception as the process through which safety and threat are detected outside conscious awareness. (Porges, 2003, 2007, 2009, 2021, 2023, 2025b, 2025a)
Where do screens enter? When a screen is used to calm the child, it offers a shortcut that bypasses the usual route through human safety cues. The child appears calmer, but co-regulation has not actually been built. Over time, this strengthens reactive pathways, so that under even minimal stress the child shifts rapidly into sympathetic explosion or dorsal withdrawal. That is why some children either erupt or disappear during transitions, noise, frustration, or change. In infancy and toddlerhood, greater background television exposure and higher overall screen exposure have been associated with poorer inhibitory control during a sensitive developmental period. (Uzundağ et al., 2026) Longitudinal evidence suggests that using media for emotion regulation in early childhood is meaningfully related to later emotional competencies, indicating that screens can become integrated into regulatory routines rather than merely serving as neutral distractions. (Coyne et al., 2023; McDaniel et al., 2026)
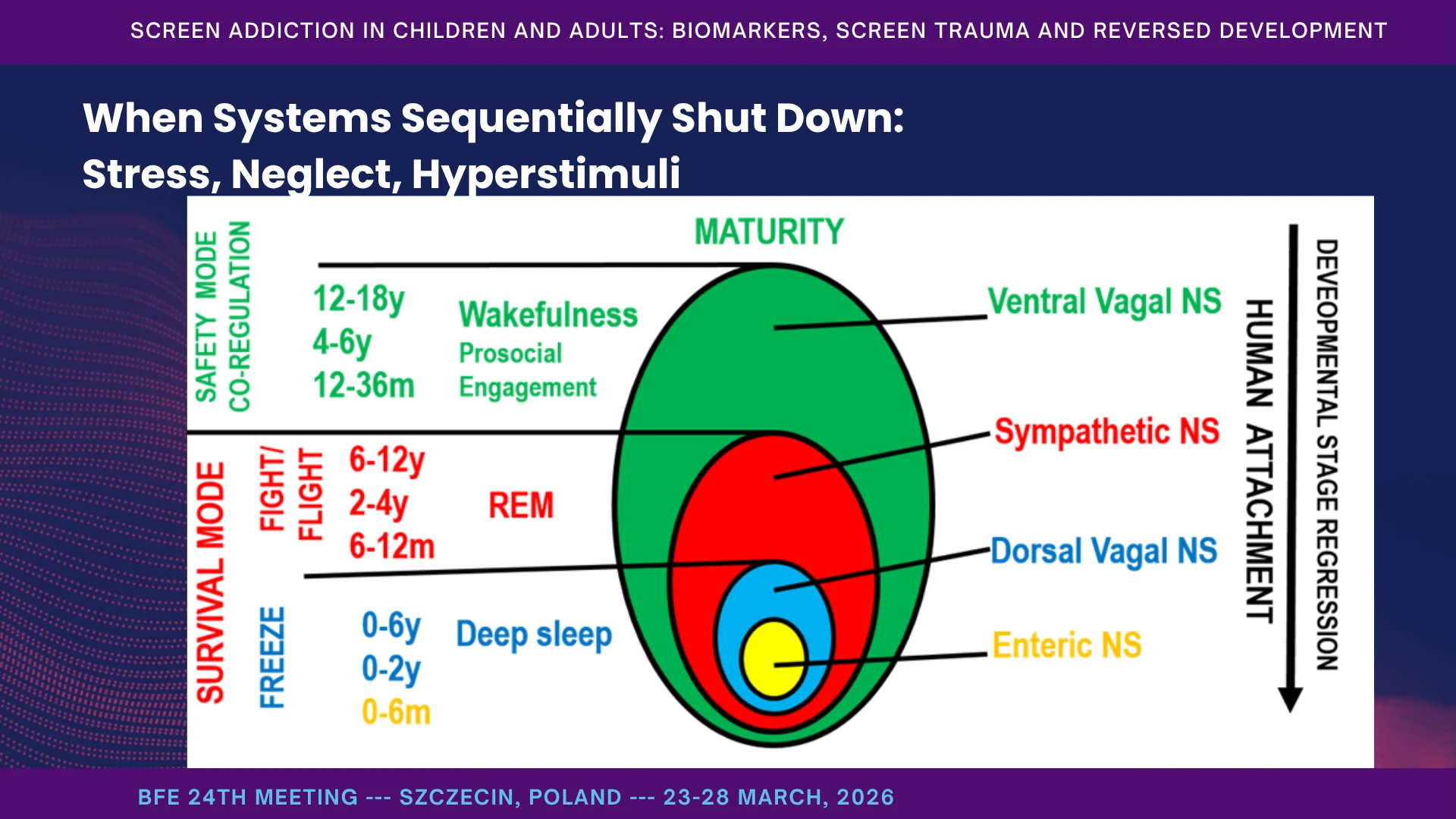
When Systems Sequentially Shut Down: Stress, Neglect, Hyperstimuli
What drives the system downward? Again and again, we see the same triggers: a lack of co-regulation at developmental crossroads - feeding, falling asleep, waking, transitions; hyperstimulation without human framing - fast videos, bright light, noise; unpredictability and chaos in daily rhythm; and pain or discomfort that is misread and then managed with a screen. Under these conditions, the ventral vagal system gives way to sympathetic activation: motor restlessness, aggression, urgency - “I want it now.” If that fails, dorsal collapse appears: vacant stare, refusal, shutdown.
The early markers are often simple but striking: a very short latency to crying or explosive reactions after minor frustration, and an inability to wait even five to ten seconds without a visual buffer. In this respect, early screen addiction can resemble severe neglect or trauma, because human co-regulation has been profoundly weakened or replaced. Parent-infant co-regulation is a key feature of the developmental niche in early life and changes systematically across infancy in relation to later social-emotional functioning. (Aureli et al., 2022)
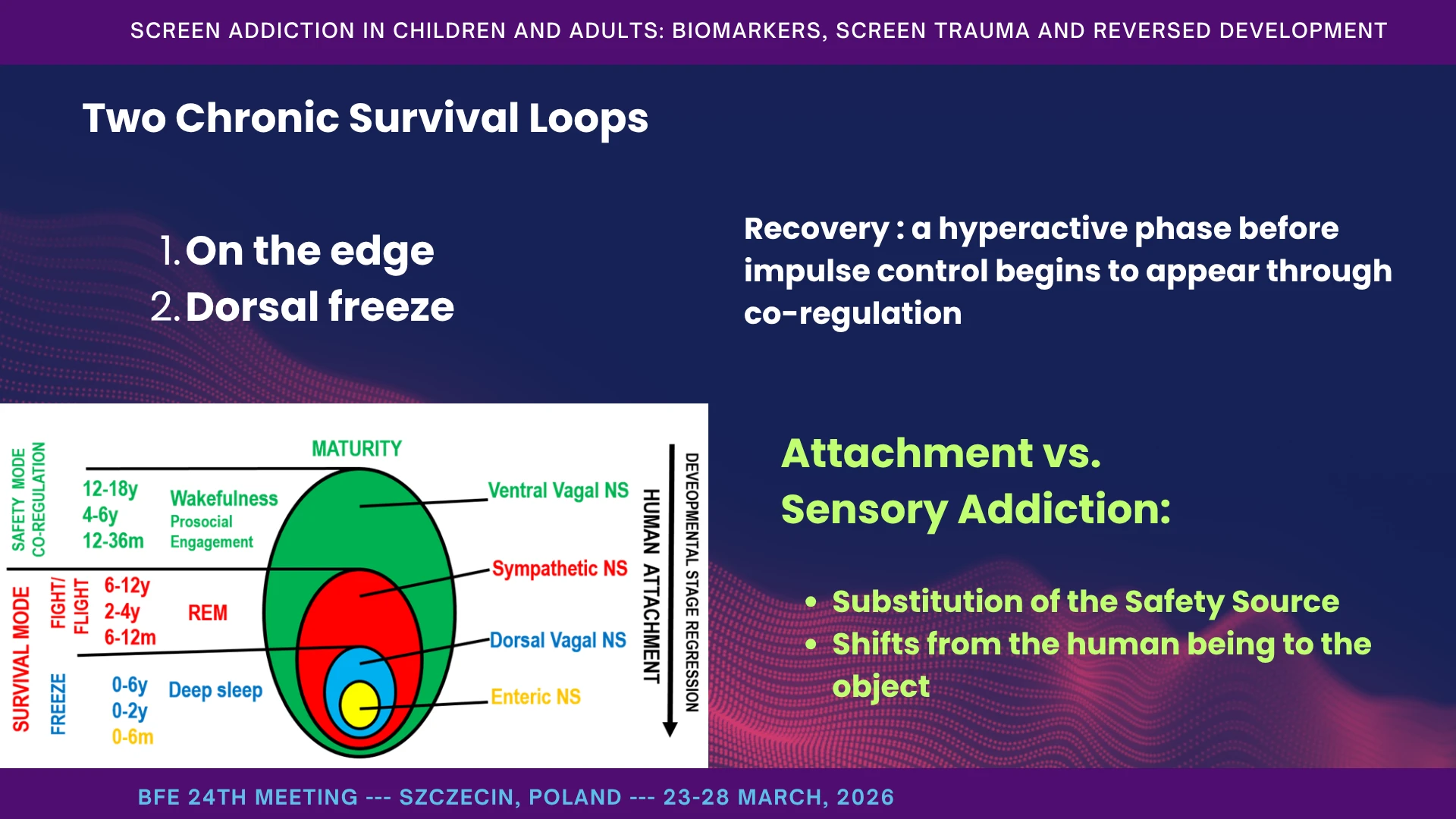
Two Chronic Survival Loops
When downward switching becomes chronic, two stable survival loops tend to emerge. The first is sympathetic dominance. The child is always on edge - loud, fast, impulsive, driven to seek continuous sensory peaks. Sleep is fragmented, transitions become battles, and the whole system lives in urgency. In this state, we often see generalized anxiety, near-panic arousal, fear reactions, hyperactivity, and growing inattention to people. Even the middle ear begins to tune more to noise than to the human voice.
The second loop is dorsal freeze. Here the child shuts down under overload, withdraws, avoids gaze, and seeks rituals of disengagement. In this state, the child may resemble a severely traumatized child: absent, unreachable, and organized around withdrawal rather than protest.
Some children move between these two states within a single day. The heavier variant is freeze and shutdown. In therapy, recovery often passes through a hyperactive phase before impulse control begins to appear through co-regulation.
When a regulatory system is missing, it must first be supplied by the social environment – by an external holding environment that co-regulates the child. As each system matures, it gradually becomes capable of self-regulation, first in routines, then in novel situations. Below these two loops, however, there are deeper levels still: reversed development, ASD-like states, and psychotic-like functioning.
Attachment vs. Sensory Addiction: Substitution of the Safety Source
Attachment is the biology of safety: gaze, voice, touch, and predictable rhythm. These are the cues that engage the ventral vagal system and support social regulation. Meta-analytic evidence indicates that greater positive parent-child synchrony is associated with stronger self-regulation across development. (Davis et al., 2017) When an infant is distressed, it is normally human signals that restore equilibrium. But if, at critical moments, a screen is repeatedly offered instead of a person, a substitution of the safety source takes place: soothing shifts from the human being to the object. The child begins to attach not to face and voice, but to rhythm, light, repetition, and sensory stimulation.
These children cannot tolerate delay. They demand “now.” They may explode when refused. There are quieter versions too: the child seems easy - but only with a screen; without it, they fall apart. This is not simply poor parenting. It is a learned association formed in the absence of impulse control: stress or change leads to screen-based stimulation, which leads to relief.
Thus, safety is sought not upward, into the human world, but downward, toward intrauterine-like states - reversing development rather than advancing it.
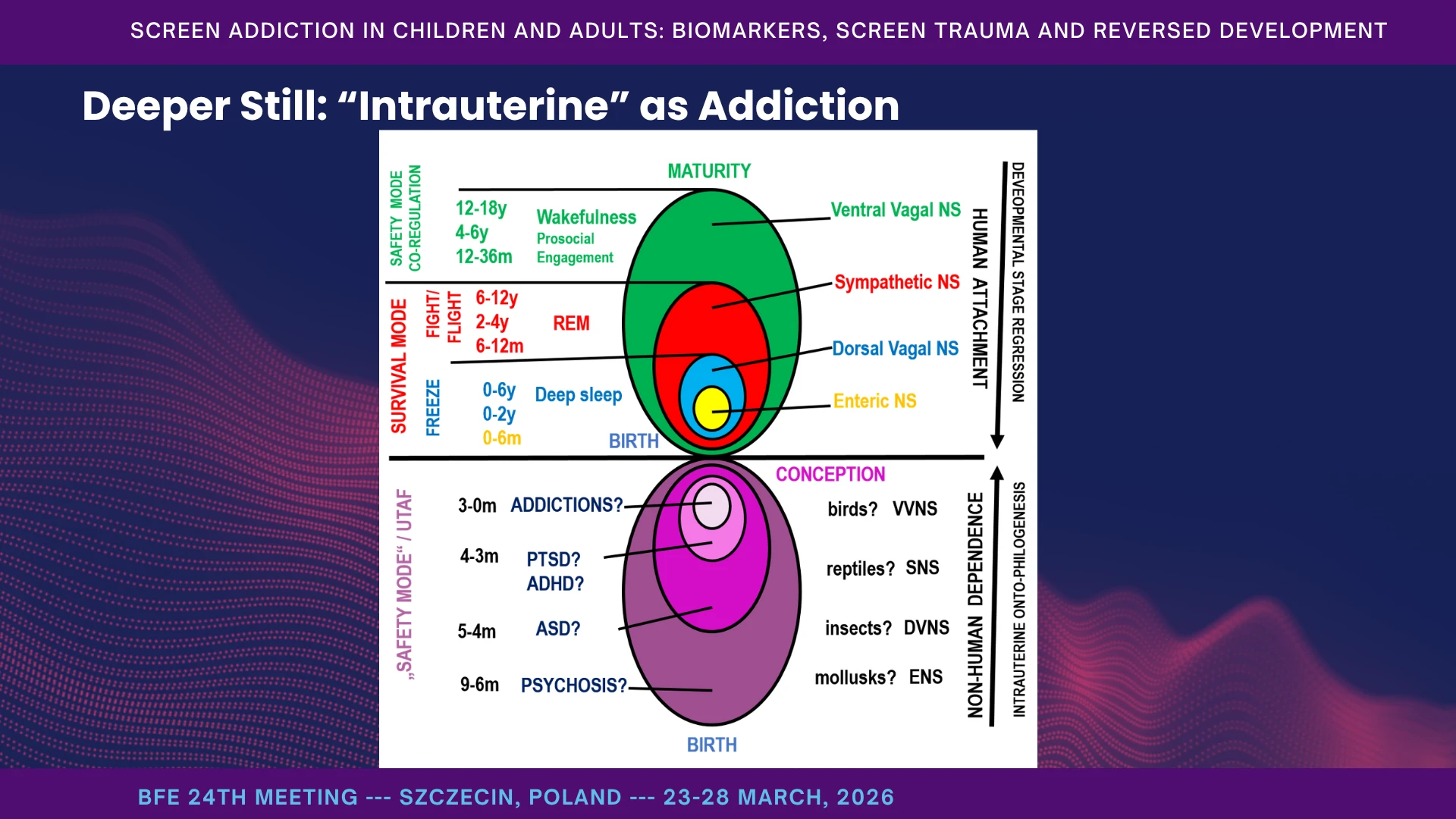
Deeper Still: The Intrauterine Pull of Addiction
A helpful image for why some children do not “return” with detox alone is this: addiction can become the nervous system’s attempt to restore a kind of intrauterine security - warmth, rhythm, predictability, enclosure - far from the complexity of the outside world. The screen offers exactly that: pulsing light and sound, constancy, and no reciprocity. When reality feels hard, chaotic, or overwhelming, the child slides inward. External developmental research is consistent with the broader importance of predictability, embodied caregiving, and contingent interaction in early life: caregiver predictability has been linked to later infant learning, and affectionate caregiver touch supports autonomic regulation, synchrony, and psychosocial development. (Forest et al., 2025)
At that point, we begin to see phenomena resembling reversed development: intense staring, self-spinning, rituals of disengagement, refusal of gaze, and eating only within a specific audiovisual script. In the deepest layers, inside and outside begin to invert: the inner film becomes more compelling than our faces, and human signals start to feel intrusive or even threatening. You speak, and the child does not truly hear you. You extend a hand, and the child does not truly see you. This is not stubbornness; it is existential defense.
Why think in this way? Because therapy must begin at the border between inside and outside, not with content. If we rush to words, demands, and rules, the nervous system retreats further inward. If we begin instead with body, rhythm, predictability, joint attention, and safe reciprocity, then the outside world gradually becomes tolerable enough for the child to emerge. This clinical observation mirrors the Neurosequential Model of Therapeutics (NMT), developed by child psychiatrist Dr. Bruce Perry, which emphasizes that interventions must align with how the brain develops and processes information - from the bottom up. (Perry, 2006a, 2006b, 2009, 2014)
Cross‑Wiring of Wakefulness/Dream‑State and Inside/Outside - A Key to Psychotic‑Like Phenomena
Another helpful clinical image is this: a cross-wiring between wakefulness and dream-state, and between internal and external reality. The child appears awake, but is functioning in dream mode: the gaze passes through us, reactions are delayed, and actions follow internal scripts - as if the child were watching an invisible film. Conversely, strong internal impulses may be experienced as external threat, leading to freeze, flight, or striking. Inside and outside begin to blend; wakefulness and dream-state start to exchange places.
Screens feed this process by bringing dream-state into the waking day: colorful, rapid, automatic streams that do not require shared attention, reciprocity, or meaning. The nervous system chooses the easier path - inward, toward automatism. And when we try to pull the child out too abruptly, the result is often collapse, because the intermediate steps are missing. Abruptly removing the screen forces the child's nervous system into the chaotic reality of the external world without any "intermediate steps". The child does not have the ventral vagal capacity (the "vagal brake") to manage the sudden transition. They collapse into dysregulation because the external object regulating their physiology was amputated before a human connection could replace it. (Schilbach et al., 2013)
The clinical observation of a "cross-wiring" between wakefulness and the dream-state perfectly captures the neurobiological phenomenon of dissociation and network dysregulation induced by chronic screen use. When a child's nervous system is tethered to a digital device, the brain's standard operating procedures for reality testing and attention are profoundly altered.
In a healthy, awake brain, attention toggles smoothly between two primary functional networks:
- The Default Mode Network (DMN): Active during internal thought, daydreaming, and self-referential processing. (Raichle, 2015)
- The Central Executive Network (CEN): Active during externally directed, goal-oriented tasks and active environmental engagement.
Screens, particularly fast-paced animations and video games, hijack this toggle switch. They induce a state of flow or hyper-focus that mimics a trance or dream-state. (Swing et al., 2010) The child appears awake, but the neural circuits responsible for active external engagement (CEN) are suppressed, while the brain enters a passive, automated state of sensory absorption. This is why the gaze "passes through" the caregiver and reactions are delayed: the child is functioning on internal scripts, actively gating out the physical world.(Van de Cruys et al., 2014)
“Reversed Development” and Evolutionarily Older Survival Reflexes
By “reversed development,” I mean a condition in which evolutionarily older survival programs begin to dominate higher human regulatory systems - not as fate, but as strategy. We see stereotyped movements such as hand-flapping and spinning, rigid ritualism, and a demand for predictability at any cost. It may appear “nonhuman,” but in fact it is a deeply human defense: when the social world becomes too complex, the nervous system shifts toward simpler automatic survival patterns.
In that state, the child begins to feel safe only in inner worlds, repetitive actions, and stable sensory routines. Other people are no longer experienced as partners in development, but as instruments for maintaining a narrow and pathological homeostasis. (Bird et al., 2024; Selman & Dilworth‐Bart, 2024)
And this is the dark paradox: such a homeostasis, governed by older phylogenetic systems, may confer real advantages to the child - reduced uncertainty, lower complexity, immediate predictability, and protection from overload. That is precisely why it can become so stable, and why therapy must understand not only the suffering it creates, but also the functions it serves. For a nervous system that feels constantly threatened or overloaded, processing human complexity requires too much metabolic energy. The pathological homeostasis of repetitive actions and screen immersion provides a tremendous evolutionary advantage in the short term: it radically lowers complexity, eliminates uncertainty, and protects the brain from sensory overload. (Friston, 2010; Van de Cruys et al., 2014)
In clinical practice, this presentation is often misdiagnosed as congenital Autism Spectrum Disorder (ASD), but researchers increasingly recognize it as a distinct acquired syndrome, sometimes referred to as "Virtual Autism" or screen-induced ASD-like phenotype. (Chen et al., 2020; Zamfir, n.d.)
Superpowers and Conservation
There is a dark paradox here: these children often display what parents experience as “superpowers.” Despite highly restricted diets (Al-Beltagi, 2024), sleep disturbance, and stereotyped sensorimotor cycles, they may appear physically robust and surprisingly resistant to ordinary illness. They often show hypermnesia, extraordinary visual recall, and remarkable stability within narrow routines. (Baron-Cohen et al., 2009; Panksepp, 1979)
They also conserve development. The child may continue to grow bodily, while the governing pattern remains frozen at an earlier stage. We see cases in which primary teeth are retained unusually long, and bowel or bladder regulation remains developmentally immature well beyond typical ages. In this sense, development is not simply delayed; it is preserved in an older configuration.
What some celebrate as divergence or neurodiversity may, in these cases, also reflect the stabilization of older, narrower modes of functioning - powerful, efficient in their own way, but costly in relation to human reciprocity, flexibility, and growth.
And this is why the problem becomes social, not only clinical. Instead of the child gradually maturing into the adult human world, the adult world begins to reorganize itself around the dependent child’s narrowed regulatory needs. That is why I call it reversed development. The question is whether we can reverse it again.
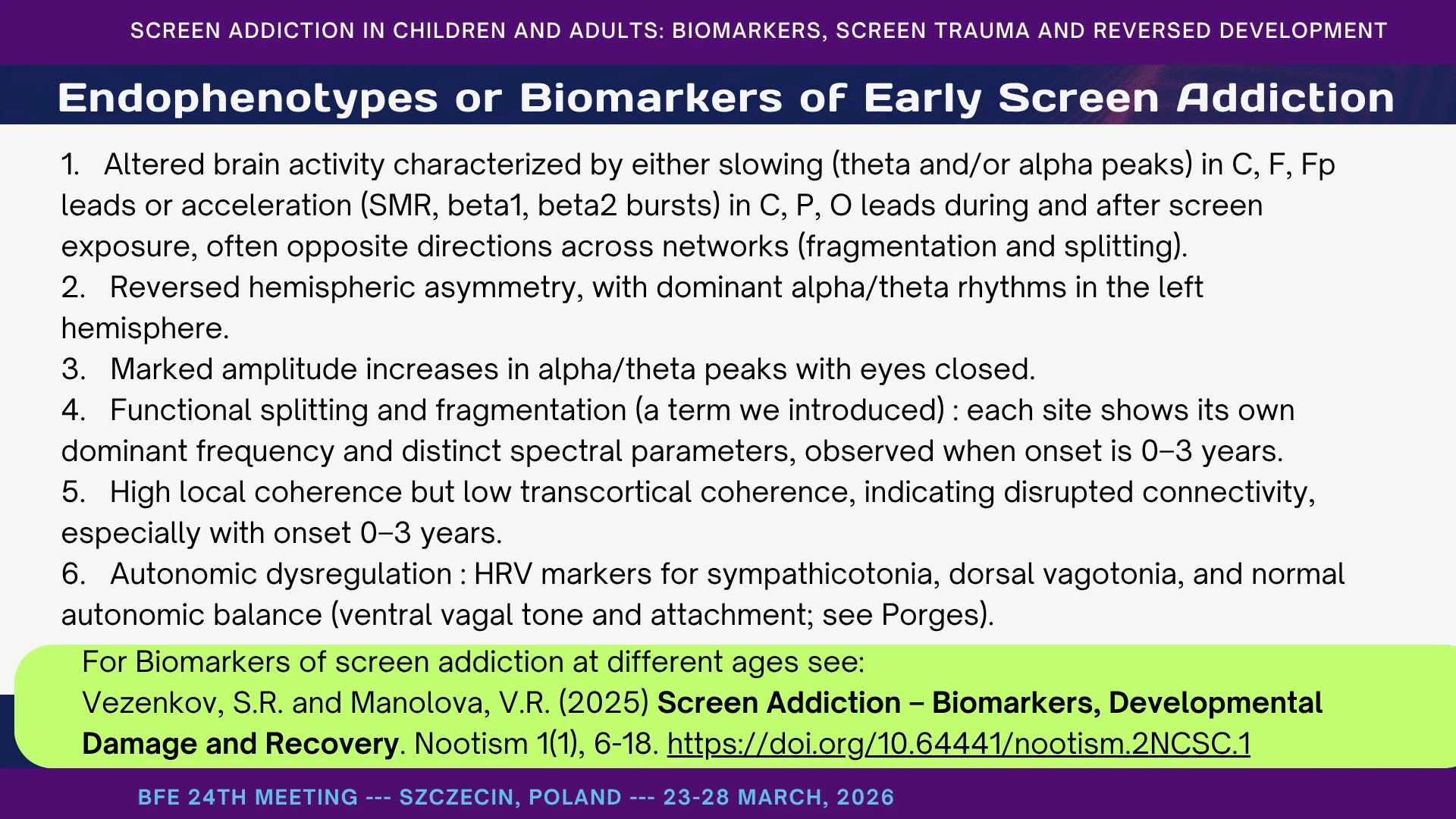
Endophenotypes or Biomarkers of Early Screen Addiction
If this framework is to be taken seriously, it must leave physiological traces. In our work, it does. We repeatedly observe four broad classes of biomarkers in children with early screen addiction and screen trauma.
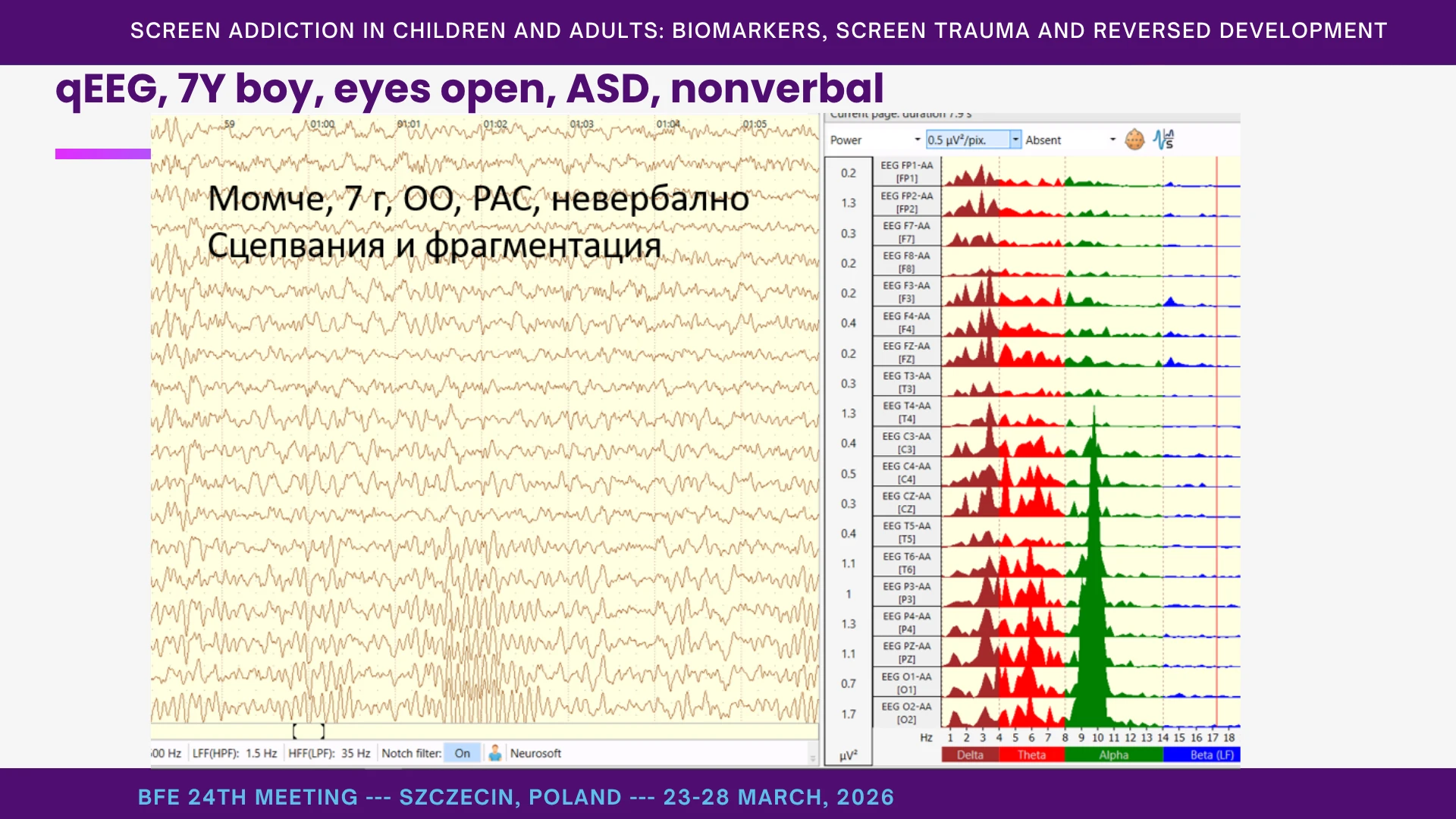
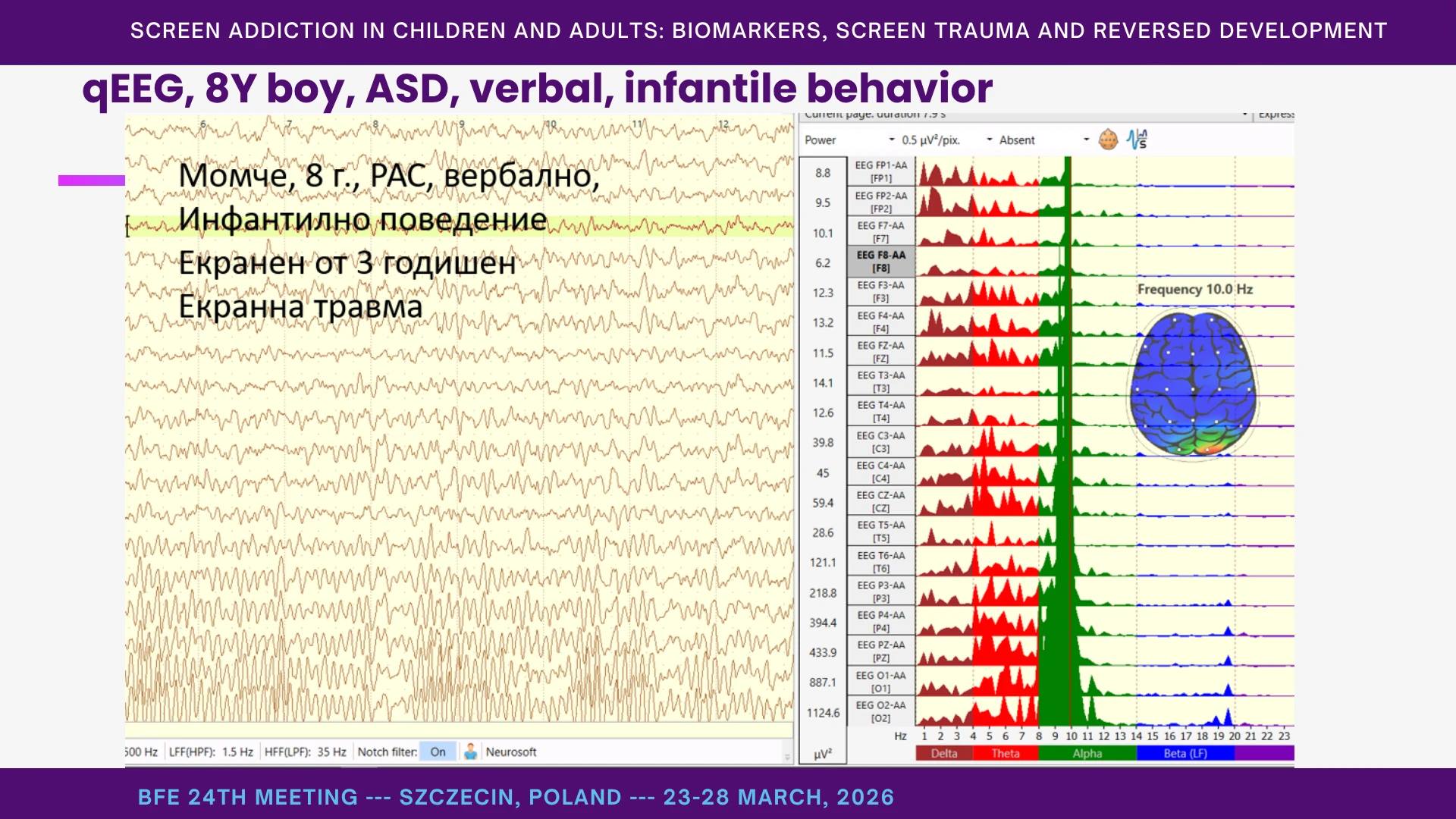
First, altered brain activity: some networks show slowing, with theta or alpha predominance, while others show acceleration, with bursts in SMR or beta ranges. Second, atypical asymmetry, including a relative predominance of alpha/theta activity in the left hemisphere. Third, fragmentation: different cortical sites begin to behave as if they are running on partially different clocks, with high local coherence but weak long-range integration. And fourth, autonomic dysregulation, reflected in HRV patterns ranging from sympathicotonia to dorsal vagal shutdown. (Lin & Peper, 2009; Peper & Harvey, 2018)
These biomarkers are not specific enough to serve as a stand-alone diagnosis. But together they outline a recognizable physiological spectrum - from nonverbal dorsal-freeze states to more verbal, high-functioning children with autistic traits. Compared with normative developmental databases, the pattern is often striking. External neurophysiological literature is broadly compatible with that expectation: studies of autism and related neurodevelopmental phenotypes have reported atypical resting-state EEG power, altered functional connectivity, and autonomic dysregulation, although findings remain heterogeneous and are not sufficiently specific for diagnostic use on their own. (Neo et al., 2023)
One methodological point is important: what is often dismissed as a mere “drowsiness artifact” may, in today’s digital developmental environment, reflect something far more meaningful. I believe this deserves re-examination. I will not go deeper into that here, but the key point is simple: these are not only markers of distorted development. They may also be markers of development being pulled toward earlier, more fragmented, and more dysregulated modes of functioning. It also supports the relevance of heart rate variability as an index of autonomic dysregulation in children and adolescents with autism-related presentations.(Bellato et al., 2022) Taken together, these findings do not define a single diagnostic signature, but they do suggest a recognizable physiological spectrum spanning more withdrawn, low-arousal states and more reactive, dysregulated profiles. (Swingle, 2019)
How Learning Systems Operate in Severe Early Screen Addiction
Learning systems - contextual/associative, instrumental, observational (mirror‑based).
System 2, System 1, and “System 0”: When Control Capitulates
To understand severe early screen addiction, we also need to ask how learning itself is reorganized. In broad terms, three learning systems are involved: contextual and associative learning; instrumental learning through reward and consequence; and observational, mirror-based learning through other people.
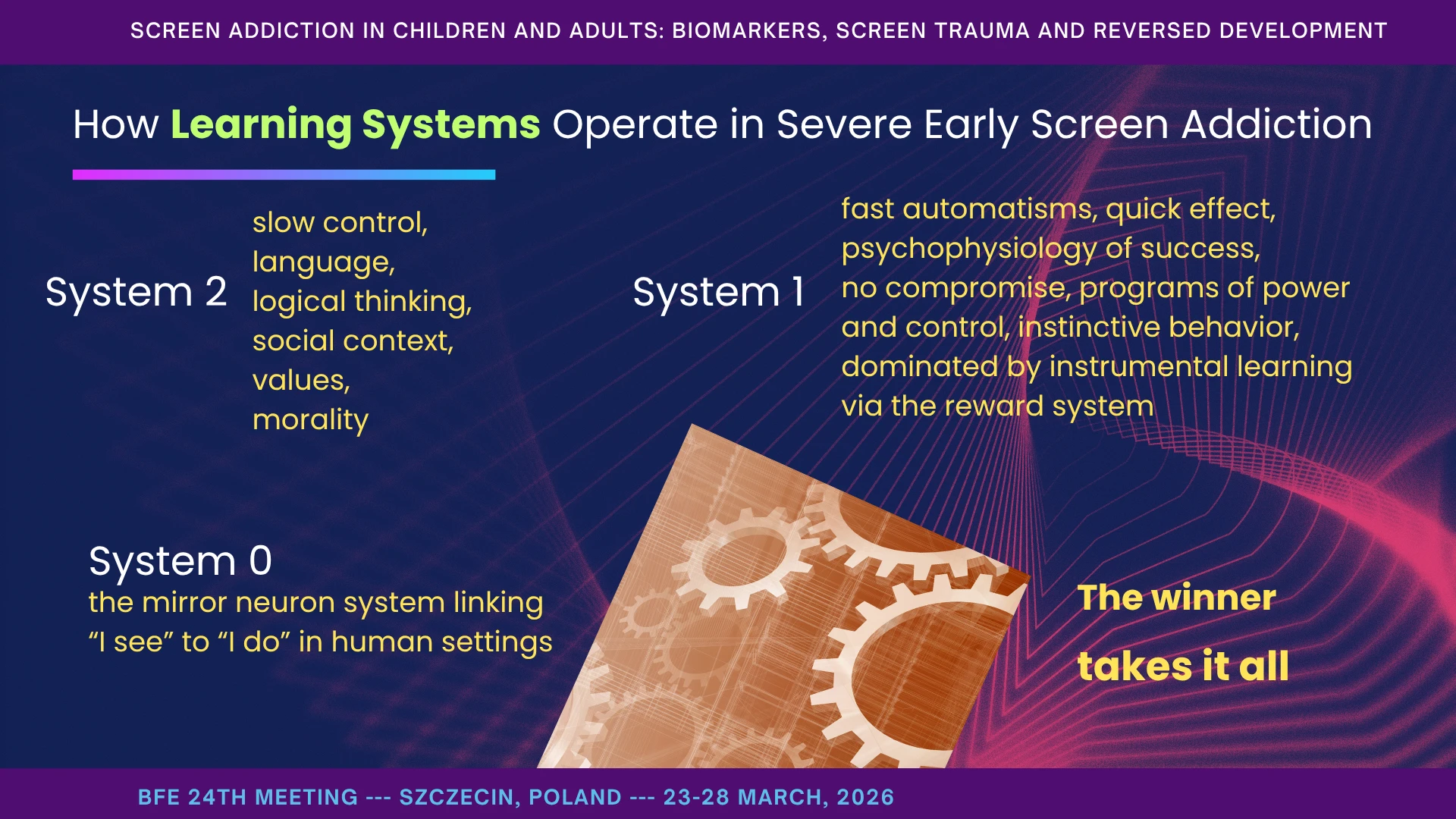
Here I use a simple working triad. System 2 /after Kahneman and Tverski/ is slow control: language, reflective thinking, social context, values, and the capacity to delay action. (Kahneman, 2011; Kahneman & Tversky, 1984) System 1 is fast control: automatisms, immediate reward, dominance, quick effect, and action programs reinforced through the reward system. And, drawing on Rizzolatti, I add what we may call System 0: the mirror system - the biological bridge between “I see” and “I do” in human settings. (Rizzolatti & Craighero, 2004; Rizzolatti & Sinigaglia, 2016)
In healthy development, these systems work together. But when the screen dominates, System 1 tends to win and close the addiction loop; System 2 weakens and stalls; (Lillard & Peterson, 2011; Strouse & Samson, 2021) and System 0 is effectively hacked - human mirroring is replaced by immersion in the object world. (Hamilton, 2013a)
Mirror Neurons (System 0): When the Screen Replaces the Human
The mirror neuron system is the biological bridge between seeing and doing. An infant watches your face and hands and, without deliberation, begins to imitate - mimicry, gesture, intonation. This “System 0” is strongest in live human encounters, because faces are three-dimensional, variable, unpredictable, and rich in microsignals.
But when the main “teacher” becomes the screen, the system becomes tuned to 2D, accelerated, edited input. Imitation does not disappear; it changes its target. The child begins to copy rapid flashes of color, shape, sound, timing, and sequence - not face, gaze, pause, rhythm, and other human microsignals. If a child hears a device-played song ten times, the stimulus is identical; if they hear a human-sung song a hundred times, it is always slightly different. One system tunes to living variability; the other tunes to sameness. Decades of developmental research have documented the "Video Deficit Effect": infants and toddlers consistently learn less efficiently from screens than from live, face-to-face interactions. (Anderson & Pempek, 2005)
Our thesis is that this effectively hacks the mirror system. It trains reactivity to artifacts rather than attunement to people. Clinically, we see the traces: weak joint attention, reduced interest in eyes and mouth, and a preference for objects, forms, and predictable audiovisual patterns. The paradox is striking: a child may imitate a cartoon character perfectly, yet be unable to follow your slow, simple gesture. Why? Because the screen delivers ready-made, perfectly synchronized patterns, while human interaction requires co-regulation. (Iacoboni & Dapretto, 2006)
At this stage, content matters less than carrier and tempo. Fast 2D light and rapid transitions do not give the mirror system enough time to hook into human microsignals. Once the child begins to experience easy victories in the screen world, the real world starts to feel too hard, too slow, and too weak. Sensory systems retune slowly, but stubbornly. That is why protection must begin early.
Recent findings suggest that mirror neurons in ASD may be less damaged than retuned. (Dapretto et al., 2006; Galli et al., 2025; Hamilton, 2013b) In our framework, the obvious question is: retuned to what? And for System 0 to work at all, the cortex must be awake - and screen addiction, as I argued earlier, tends to pull it toward dream-state functioning.
Immediate Reward: “Hacking” System 1 and Instrumental Learning
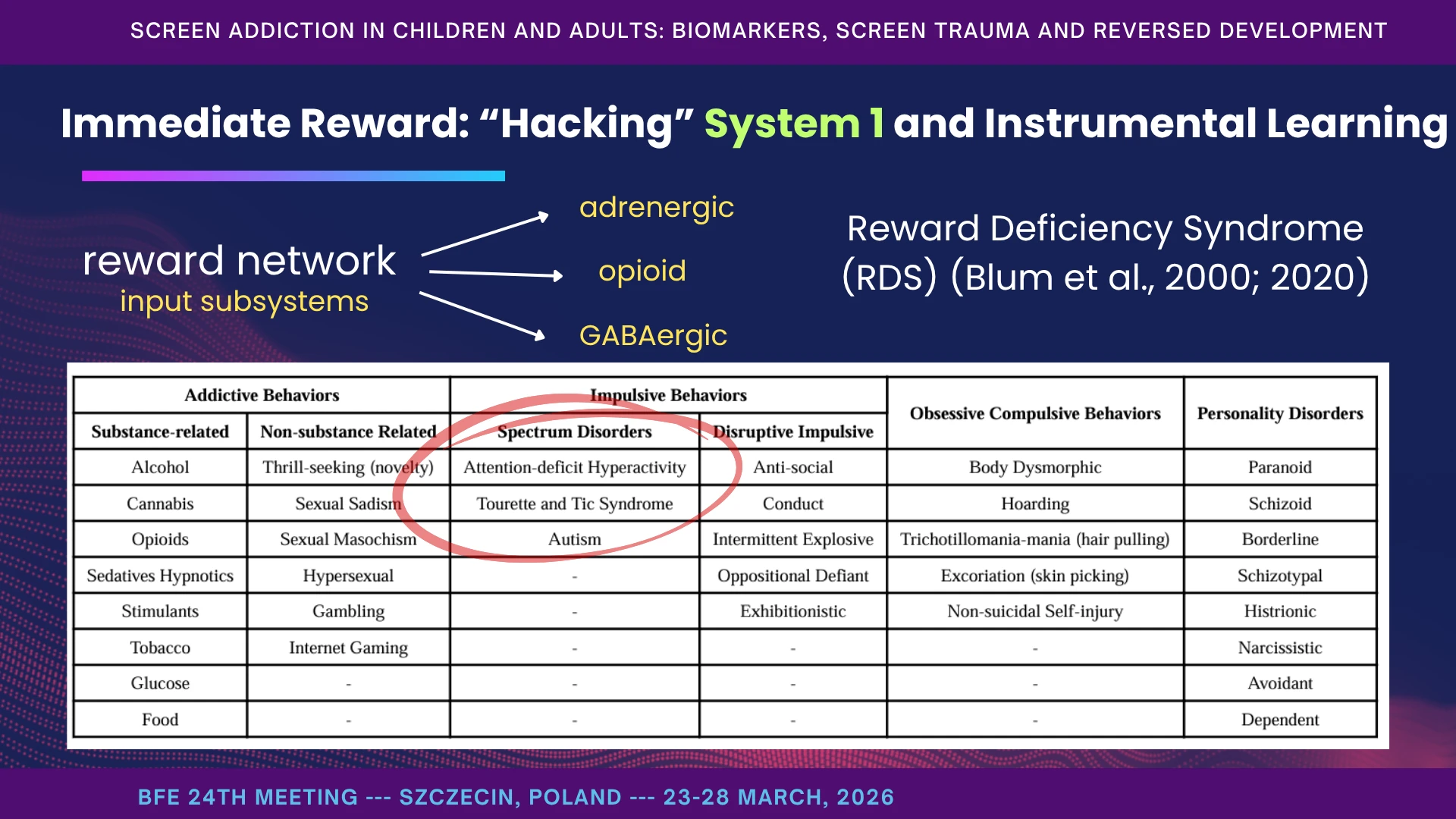
If System 0 explains how the child stops learning from people, System 1 explains why the screen becomes so hard to resist. Instrumental learning is built on immediate reward. When an action reliably produces a highly desirable outcome, the brain automates that action. In the context of early screen exposure, the device provides an overwhelmingly powerful, artificially engineered reinforcement loop that fundamentally alters the child's neurochemistry. The reward network does not depend on one chemical alone; it integrates arousal, pleasure, relief, and inhibition - adrenergic, opioid, and GABAergic subsystems converging on dopaminergic reinforcement. (Galaj & Xi, 2021; Volkow et al., 2019) Dopamine is not the chemical of pleasure; it is the chemical of seeking, craving, and anticipation. Screen algorithms (like auto-playing videos and variable-reward games) perfectly exploit the brain's mesolimbic dopamine pathway (the nucleus accumbens). This creates a compulsive drive to keep watching or swiping, seeking the next novel stimulus. In other words, the screen is not just seen; it is felt as a fast regulatory success. (Dresp-Langley, 2020b; León Méndez et al., 2024; Mathiak & Weber, 2006)
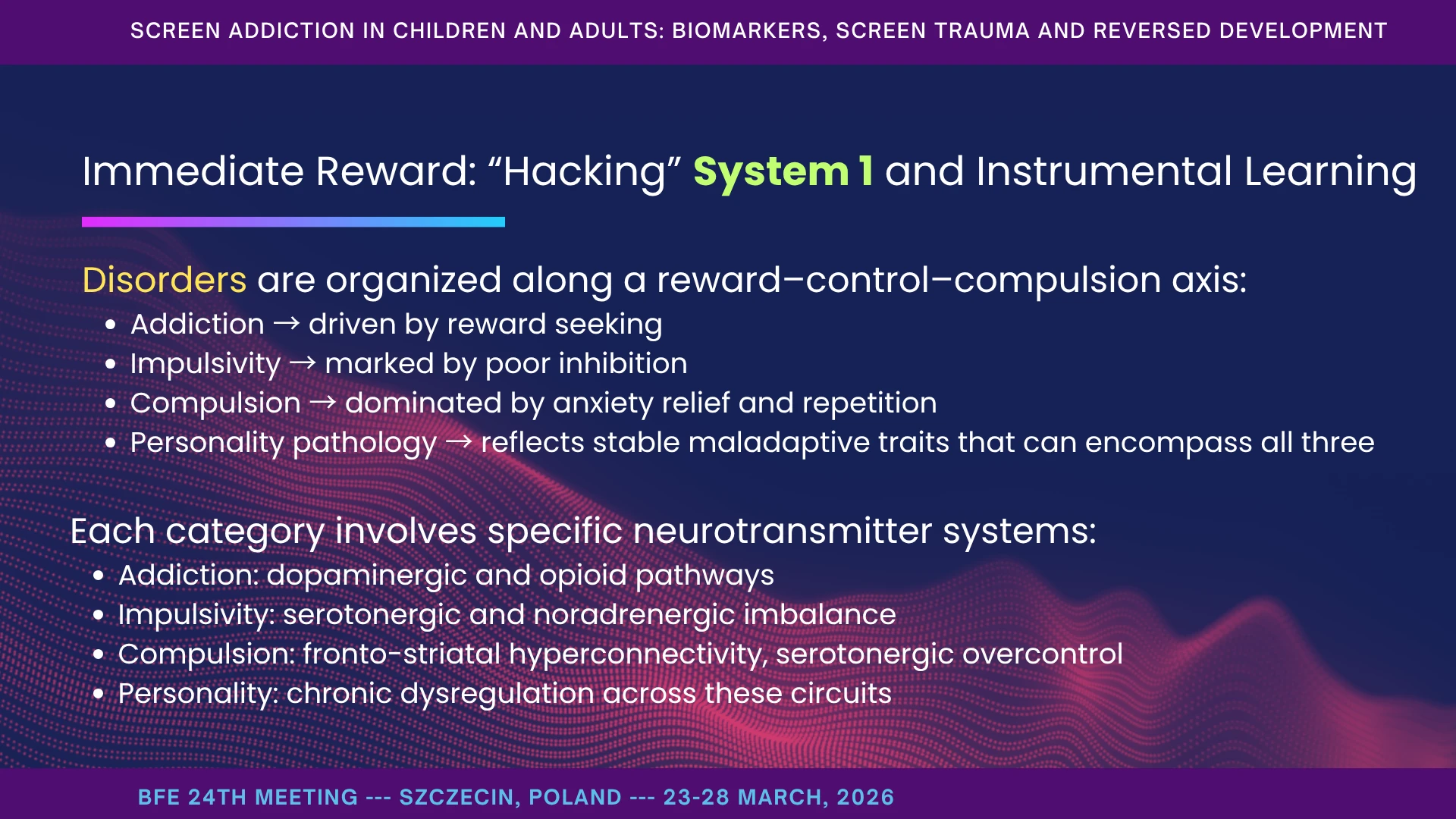
Blum’s framework helps place this within a broader neurobehavioral spectrum. (Blum et al., 2000, 2020) Addiction, impulsivity, compulsivity, and even personality-level maladaptation are not isolated boxes; they lie along a shared reward–control–compulsion axis. Addiction is driven by reward seeking. Impulsivity reflects poor inhibition. Compulsion is dominated by anxiety relief through repetition. And more stable maladaptive personality patterns may contain elements of all three. (Koob & Volkow, 2016)
That matters here because screen addiction recruits the same logic: rapid cue, rapid reward, rapid relief, repeated again and again. The child does not simply “like” the screen. The screen becomes the fastest available pathway from tension to regulation, and from uncertainty to predictable reinforcement.
So when I say that System 1 is being hacked, I mean that instrumental learning itself is being reorganized around immediate reward.
Hypo- OR hyper- executive loops
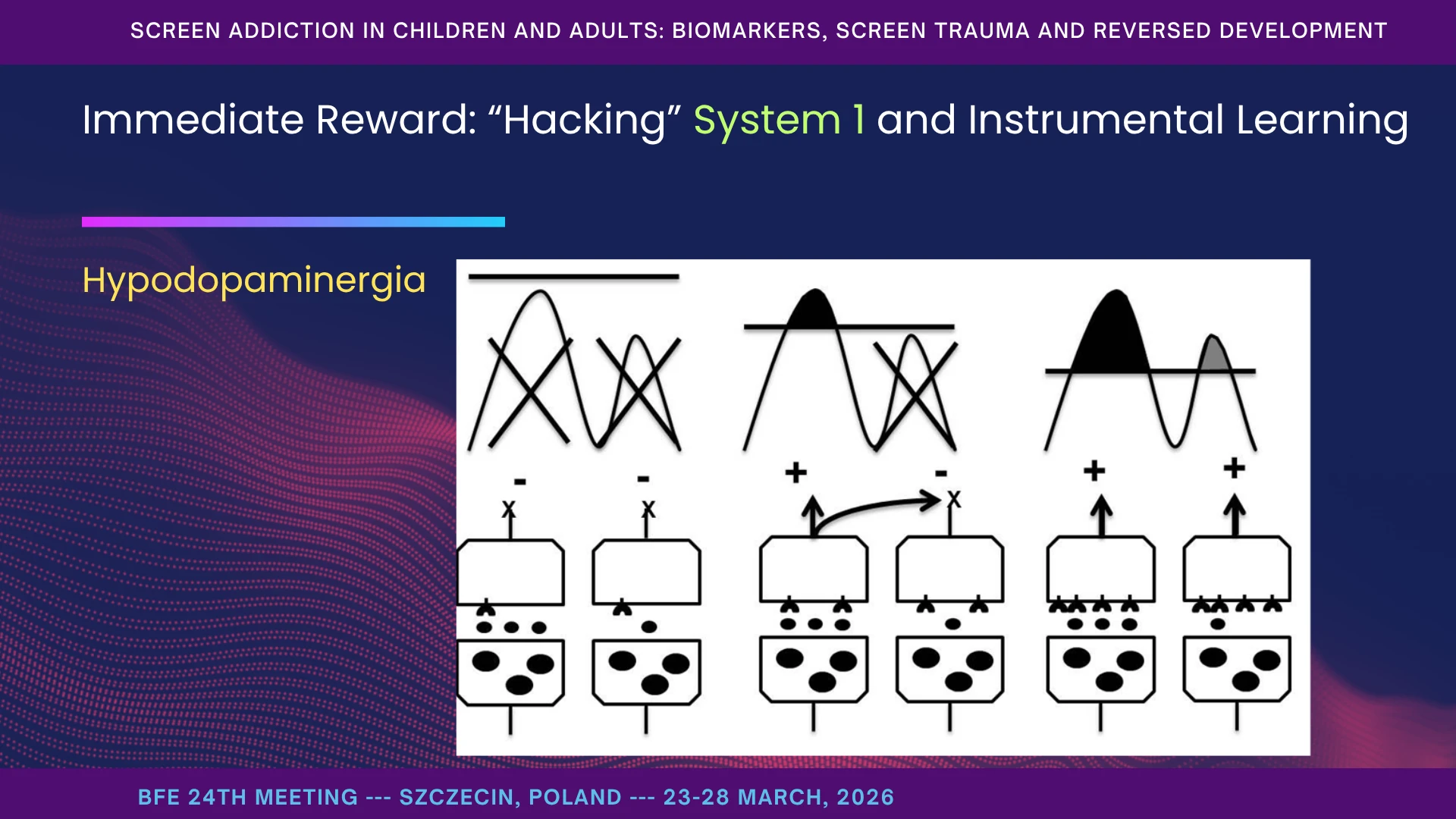
This figure helps us think about dopamine not simply as a reward signal, but as a gating signal. Within the cortex–basal ganglia–thalamus–cortex loops, dopamine helps determine which motor and cognitive programs are facilitated, which are inhibited, and which are allowed to pass into action. In that sense, it is a mediator of selection. (Mink, 1996; Volkow et al., 2011)
The basal ganglia act as the brain's central clearinghouse for behavior. When the cortex formulates an intention (e.g., "pick up the block" or "look at the parent"), the signal must pass through the basal ganglia to be authorized or "gated" into action. This gating occurs via two primary, opposing pathways:
- The Direct Pathway ("Go"): Facilitates the selected action.
- The Indirect Pathway ("No-Go"): Inhibits competing or inappropriate actions.
Dopamine dictates the balance between these two pathways. Dopamine D1 receptors excite the "Go" pathway, while D2 receptors inhibit the "No-Go" pathway. In a healthy, regulated nervous system, dopamine smoothly releases the brake on the desired action while keeping the brakes firmly clamped on distracting impulses.
If dopaminergic tone is too low in systems responsible for action selection, we may see underactivation, rigidity, tics, facial grimacing, or difficulty initiating and stabilizing appropriate programs - in a Parkinsonian-type model. If dopaminergic regulation becomes excessive or unstable, we may instead see abrupt mood shifts, rapid behavioral switching, compulsive sensory seeking, and poorly gated impulses - in a schizophrenia-spectrum model.
I am not suggesting that these children simply “have Parkinsonism” or “have schizophrenia.” The point is theoretical: the same dopaminergic architecture helps explain why some children become rigid and under-responsive, while others become over-reactive, unstable, and driven by compulsive seeking. (Maia & Frank, 2011)
Ultimately, the CBGTC loops do not operate in a vacuum; they require top-down supervision from the Prefrontal Cortex (System 2). However, as discussed earlier, early screen trauma stalls the development of the prefrontal cortex.
When the prefrontal cortex fails to provide executive oversight, the child is left entirely at the mercy of subcortical dopaminergic fluctuations. The child does not "choose" to be rigid or explosive; they are trapped in a malfunctioning neuro-computational loop where the very chemistry required to select an action, stabilize a mood, or inhibit an impulse has been fundamentally destabilized. (Arnsten, 2009)
This is not the whole story, but it gives us a crucial map for thinking about motivation, action, and cognition when executive gating begins to fail.
System 2 - Language, Logic, Values, and the Human Self
System 2 is the level of language, logic, values, and the human Self. There are direct connections between the prefrontal cortex - the seat of the Self - and cardiac regulation, reflecting autonomic balance when the ventral vagal system and attachment systems are engaged (Thayer et al., 2009). In other words, the human Self does not develop in isolation; it is built in relationship. It is shaped by social experience, family life, tradition, and the broader culture - but most profoundly by the immediate relational environment.
Under survival conditions, however, prefrontal regulation gives way, and older subcortical systems assume control. That is why a child may know words, even scripts, yet fail to use them for reflection, reciprocity, or moral orientation. (Arnsten, 2009)
When screen stimulation dominates, System 1 prevails and closes the addiction loop. System 2 weakens or stalls, so even when social skills appear trained, they often function within an addictive framework rather than a truly relational one. Meanwhile, System 0 is hacked: human mirroring and reciprocity are replaced by immersion in objects and artificial stimuli.
That is why the deepest damage is not only behavioral. It is damage to the conditions under which the human Self comes into being.
Sensory Disintegration, Splitting, and Cortical Fragmentation: Two Ages in One Body
By sensory disintegration, I mean the failure of sensory streams to come together into shared meaning in real time. The child both hears and sees, yet cannot extract what is relevant for action (Feldman et al., 2018). And by cortical fragmentation, I mean something we observe clinically again and again: different behavioral and attentional systems seem to run at different speeds. Visual reactivity is ultrafast and insistent, while frontal control remains slow and fragile. The result is tunnel attention to light and motion, together with a collapse of responsiveness to social cues, which require slower integration and adaptive regulation (Just, 2004; Lage et al., 2024).
This is why we often see what I call “two ages in one body.” A child may solve a complex puzzle yet be unable to wait a turn; quote entire lines yet fail to request water; sit calmly with a tablet yet resist sitting at a table. This is not contradiction. It is context dependence built on fragmented networks (Cahalan et al., 2025).
These phenomena become especially visible under cognitive load or during transitions. When the system is overloaded, higher functions - language and executive control - drop out first, and older circuits take over: stereotypies, fight-or-flight reactions, freeze, or phylogenetically ancient survival patterns. During transitions, fragmentation appears as task collapse: the child seems to “forget” what they were doing, as if no functional bridge connects the previous state to the next one (Happé & Frith, 2006; Pastor-Cerezuela et al., 2020).
What Is “Screen Trauma” and Why Detox Alone Fails
By “screen trauma,” I mean a durable retuning of regulatory and sensory systems such that even after screens are removed, the child remains anchored in infantile, sensory-dominant patterns. Why does detox alone so often fail? Because many behaviors formed in dream-state, under immediate reward, do not dissolve automatically when the environment changes (Uzundağ et al., 2022).
What remains are developmental anchors: screen-induced pathological reflexes, vestibular and postural distortions, sensory disintegration, and cortical fragmentation with vision-dominant processing. These anchors pull development backward under load, change, and stress (Chisari et al., 2024a; Manolova & Vezenkov, 2025e, 2025a; Vezenkov & Manolova, 2025e, 2025d, 2025f).
The child’s functioning becomes tuned to stereotyped, repetitive stimuli on which they have become dependent, rather than to a changing environment that requires constant adaptation. Lacking that adaptive capacity, the child regresses under even minimal challenge into anxious explosion, hysteria, shutdown, or intrauterine-like withdrawal - states in which there is no learning, only survival (Manolova & Vezenkov, 2025e, 2025g).
That is why the next question is not only whether a child has been detoxed, but what developmental anchors still remain. Let me now show you some of the anchors we have identified.
A Developmental Anchor: Screen-Induced Pathological Vestibular Reflex - SIPVR
Let me show you one of the developmental anchors we repeatedly observe: what we call the Screen-Induced Pathological Vestibular Reflex, or SIPVR. When a typically developing child is gently inverted, without additional contact support, the response is usually relaxed and often even playful - laughter, curiosity, trust in the adult’s hold.
In contrast, in many children with early screen addiction, including children carrying an ASD diagnosis, we observe a very different pattern: arching backward, reaching frantically for support, trembling, panic, whole-body muscular rigidity, and intense fear of falling. This is not simply dislike. It is a pathological vestibular reaction (Vezenkov & Manolova, 2025e).
What is especially important is that the reflex often diminishes as soon as the child can grasp something stable - clothing, a leg, a hand, or the ground. In other words, regulation returns only when visual or tactile anchoring is restored.
That is why we consider SIPVR not just a symptom, but a developmental anchor: a sign that balance, safety, and sensory integration have been pathologically reorganized, with visual input assuming dominance over vestibular processing.
In children with autism, postural-control differences have been repeatedly reported, especially when sensory information is altered, and recent work suggests that sensory-system integration for balance may be less developed even when peripheral vestibular function itself is not grossly abnormal. In parallel, the sensory-integration literature describes gravitational insecurity as a vestibular-based dysfunction marked by exaggerated fear, avoidance, and postural-emotional responses during movement or changes in head position (Chisari et al., 2024a).
Watch the video:
0–20 s – In the first part of the video, you see a typically developing child during the inversion test. When gently lifted upside down, the body remains relaxed, breathing stays steady, and the expression is curious or even playful. There is trust - in gravity, in the adult’s support, and in the child’s own vestibular system. This is what a healthy vestibular response looks like: posture, balance, vision, and safety are working together.
20–45 s – Now observe the contrast. In the second child, we see immediate muscle tension, arching backward, and frantic grasping for support. Instead of playfulness, there is panic. This is not simply dislike or surprise. It is a defensive reflex. The nervous system interprets inversion as danger because visual input has come to dominate vestibular processing.
And notice the key point: as soon as the child touches something stable - or regains visual orientation - the panic begins to subside. That is why we call this SIPVR: the child calms only when visual or tactile anchoring is restored. In our view, this is not just a symptom. It is a developmental anchor, showing how early audiovisual overstimulation can override vestibular trust and keep regulation at a reflexive rather than a relational level.
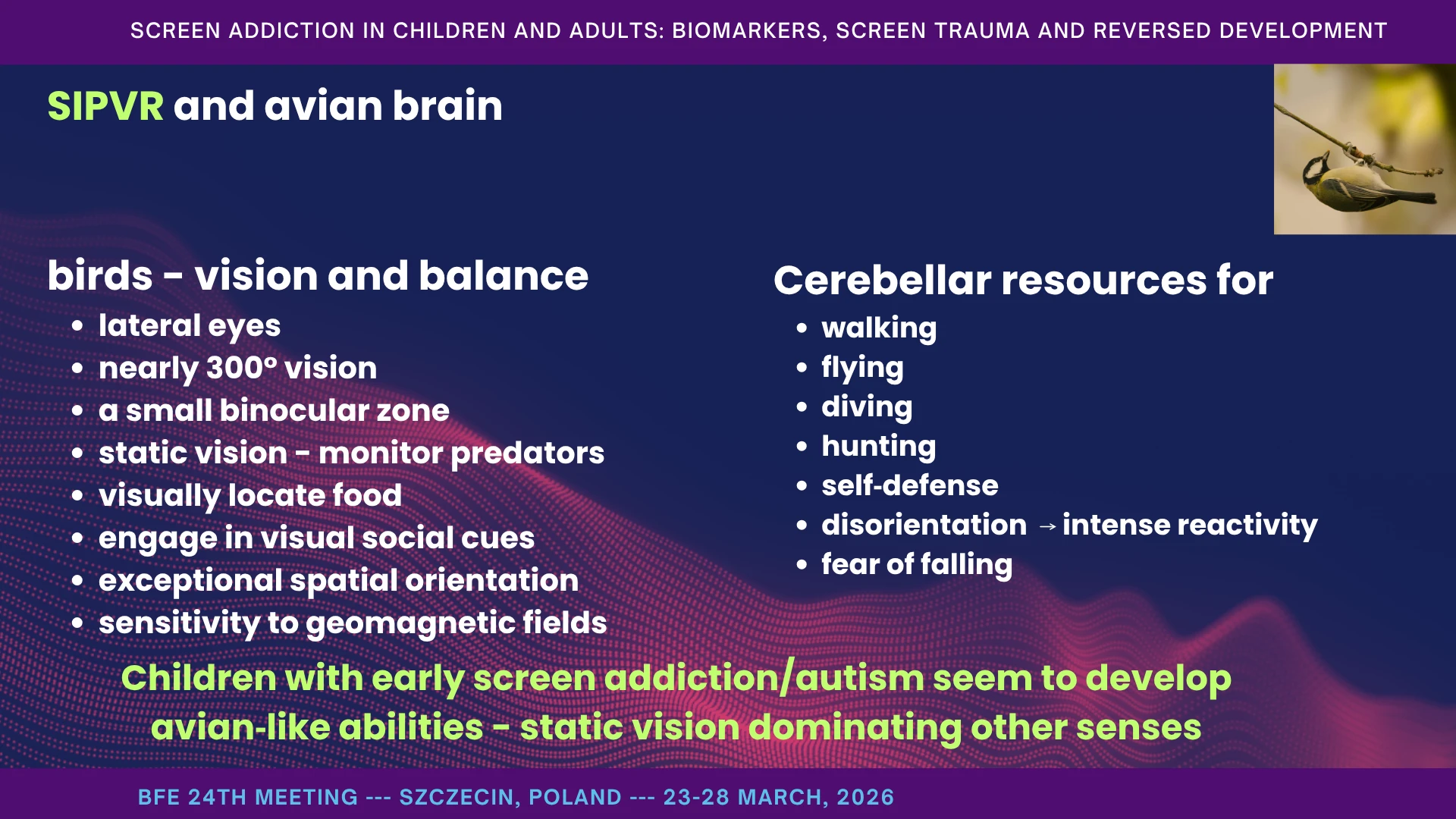
Vision-dominant regulation: an avian analogy
This next observation helps us understand what vision-dominant regulation can look like. When certain animals - especially birds - are turned upside down, they instinctively rotate the head in order to restore horizontal visual orientation. In highly visual species, balance and orientation are tightly coupled to vision. A substantial part of cerebellar function supports exactly this: keeping the head and sensory frame aligned during movement, flight, diving, hunting, and self-defense. When that alignment fails, disorientation and intense reactivity follow.
Birds offer a useful analogy here, because the avian brain is profoundly vision-centered. Much of its behavior is organized around visual monitoring, spatial orientation, and rapid environmental mapping. I am not saying these children become “bird-like” in any literal sense. I am saying that, in some of them, we observe a strongly vision-dominant profile: visual input begins to override other sensory systems (Wylie et al., 2018).
Clinically, this can look striking. Some children with early screen addiction, including children carrying an ASD diagnosis, show extraordinary spatial orientation and unusually strong visual recall. They may see a pattern once and retain it immediately - an alphabet, an arrangement, a route - without understanding or caring about its meaning. For them, it is not language or symbol; it is a visual configuration (Chisari et al., 2024a; Chung & Son, 2020).
That is the key point: what appears as a gift may also be a sign of narrowing. A function sharpens, but the whole child does not necessarily develop. Visual power increases, while multisensory integration, reciprocity, and flexible meaning-making weaken (Chung & Son, 2020).
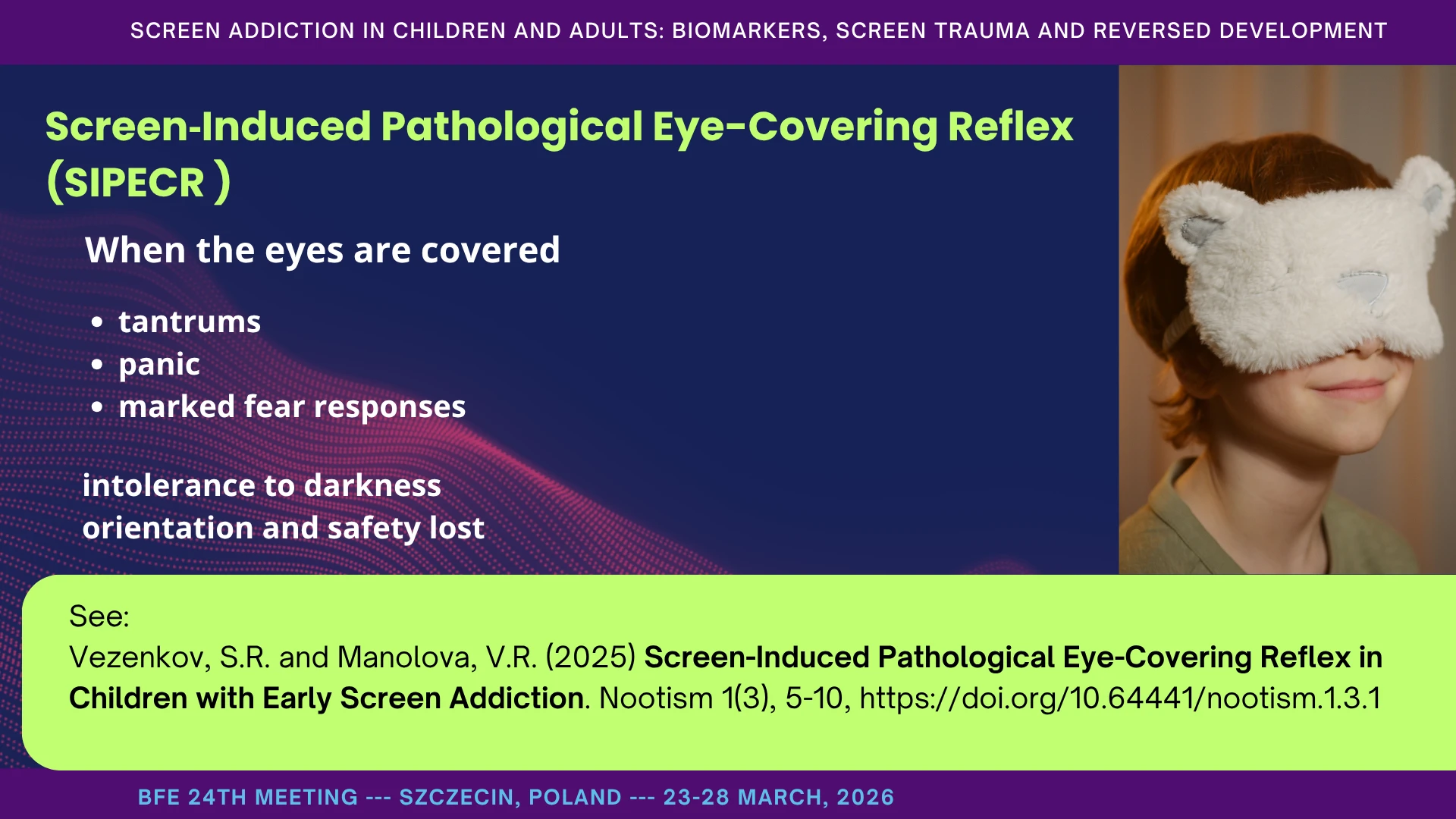
SIPECR - Screen-Induced Pathological Eye-Covering Reflex
A second developmental anchor is what we call SIPECR - the Screen-Induced Pathological Eye-Covering Reflex. When the eyes are covered, whether by hands, a mask, or a cloth, the reaction is often immediate and intense: tantrums, panic, and marked fear responses. In our clinical observations, this occurs in the great majority of cases. (Vezenkov & Manolova, 2025d)
These children also tend to show a marked intolerance to darkness, whether during rest or sleep. This is clinically important, because it suggests that vision has taken on a dominant regulatory role. When visual input is suddenly removed, the nervous system does not simply lose information - it loses orientation and safety.
In that sense, SIPECR is not just a behavioral oddity. It is another developmental anchor, showing how strongly regulation has become dependent on visual control of the environment.
Other older phylogenetic reflexive patterns
Beyond SIPVR and SIPECR, we observe a broader cluster of what may be called evolutionarily older survival patterns. These are not isolated curiosities. They form part of the developmental anchors that keep the child organized around reflexive safety rather than social growth (Chisari et al., 2024b; Manolova & Vezenkov, 2025a; Vezenkov & Manolova, 2025e, 2025d).
Some are vestibular: absence of nystagmus during rotation with the eyes open, asymmetry between left and right rotation, or marked intolerance to even mild thermal airflow near one ear. Others are visual-postural: a characteristic angled gaze, with slight head tilt and prolonged fixation on a single point or light source (Ornitz, 1974).
We also see disturbances in body mapping. Gentle separation of the toes - or sometimes the fingers - can trigger an unexpectedly intense reaction, often strongest at the little toe. Clinically, it can feel as though individual digits are not represented in a differentiated way, but are experienced as one undivided unit.
Motor patterns may also shift toward older survival forms: primitive repetitive tongue movements, head-down charging patterns, rapid flapping-like arm movements, chaotic finger activity, and episodes of pinching, scratching, or biting of extreme intensity. In some cases, the physical strength shown during attempts at restraint is strikingly disproportionate for the child’s age.
These are markers of what we call reversed development - not retained primitive reflexes, and not merely regression to earlier developmental stages, but an environmentally induced descent into an intrauterine-like state in which older phylogenetic programs begin to govern development, pulling it onto a trajectory fundamentally different from typical human development.
That is why all therapeutic work is shaped by this context. These patterns do not influence the child alone; they come to organize the family, and eventually even the therapeutic and educational environment around themselves.
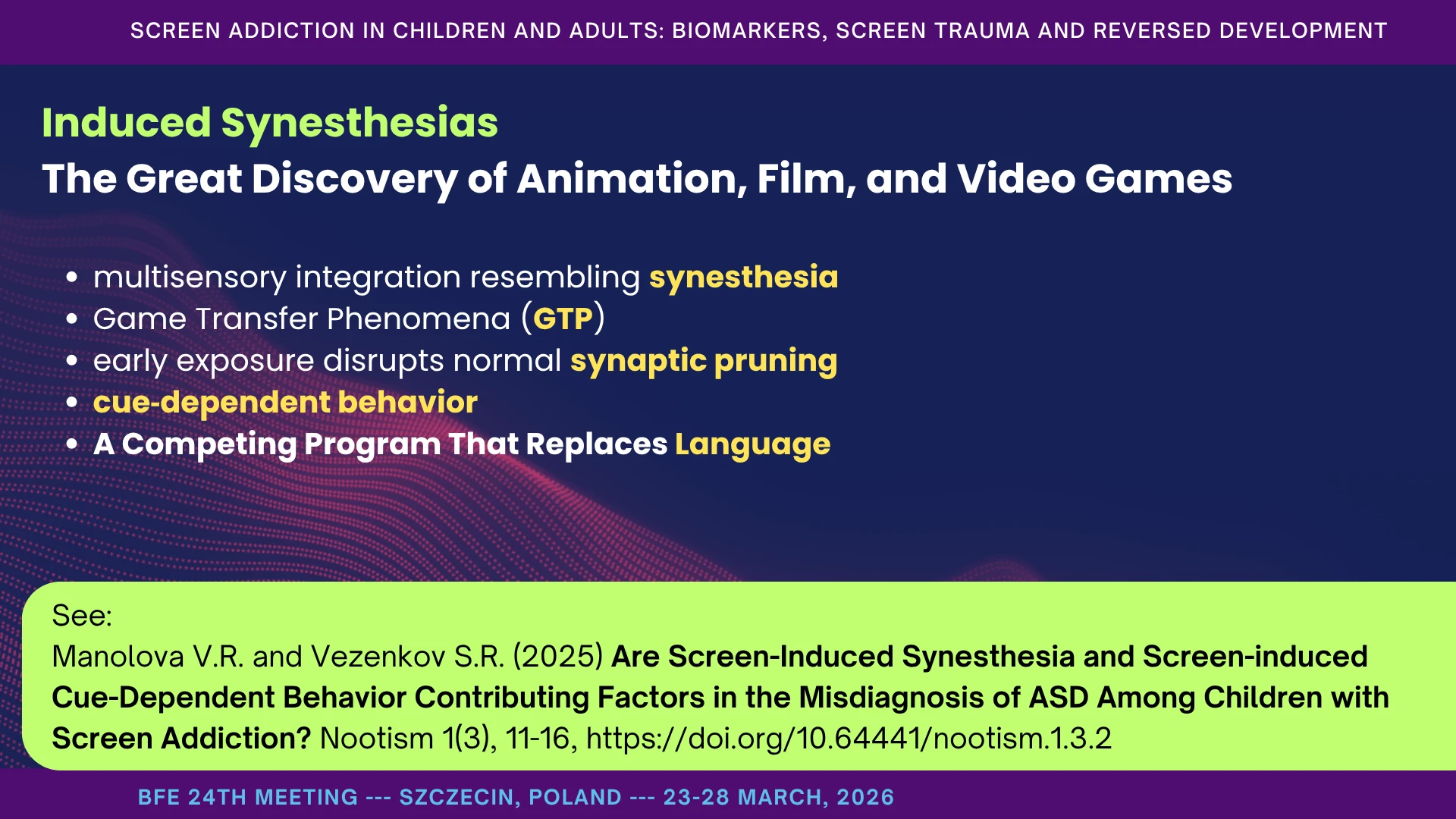
Induced Synesthesias - The Great Discovery of Animation, Film, and Video Games
A further developmental anchor is what I call induced synesthesia - or more carefully, synesthesia-like multisensory coupling. Animations, films, and video games are structured to maximize tightly coupled audiovisual immersion: color, movement, rhythm, sound, and emotion are bound together into one sensory event. In vulnerable developmental periods, that kind of coupling can become a powerful organizer of perception and behavior (Manolova & Vezenkov, 2025a).
Neurodevelopmentally, the concern is not only overstimulation, but retuning. Early repetitive exposure may bias pruning toward visual and associative systems, weaken cognitive flexibility, and produce cross-sensory rigidity: eating only with a specific visual cue, sleeping only with a certain song, calming only with a known audiovisual sequence. In some children, these patterns may then be mistaken for core ASD-like symptoms.
Dreaming is one state in which cross-sensory blending becomes especially prominent. My working hypothesis is that screen addiction brings dream-state organization into waking life. The child is awake, but perception begins to behave as if it were organized by dream logic: visual input dominates, and through it other modalities - taste, temperature, proprioception, even pain - are more easily recruited into one fused loop.
That is why old animations matter. What you see in Flowers and Trees is not just an artistic breakthrough. It is an early demonstration of media learning to speak directly to the nervous system - binding color, movement, music, and emotion into a single immersive circuit. It is beautiful, and it is powerful. But the same principle, scaled and intensified in modern animations and games, can trap the child in multisensory loops where perception, emotion, and compulsion begin to fuse.
Watch the video:

A Competing Program That Replaces Language
Language is not simply replaced by silence. It is often replaced by a competing program. Early screen addiction in the first two years of life is strongly associated with severely disrupted language development - not because the child does not hear words, but because words are no longer embedded in human context.
What appears instead can sound deceptively rich: echolalia, scripts from songs and clips, counting, rhyming, naming colors, fragments of dialogue. But these forms are not used for requesting, sharing, responding, or building joint meaning. They are repeated, not inhabited (Mateev, Manolova, et al., 2025; Vezenkov & Manolova, 2025b).
At the same time, the real foundations of language are often missing: gestures, pointing, bringing, triadic gaze, serve-and-return exchanges, pausing, turn-taking, and attunement to another person’s prosody. The child may produce verbal output, yet fail to follow simple human commands such as “give,” “show,” or “come.”
That is why I call it a competing program. The screen supplies a ready-made rhythm, ready-made intonation, and ready-made sequence, and these begin to substitute for the slow social construction of language. What grows is not language in the full human sense, but an audiovisual script that occupies its place.
Screen Detox – Reintroducing Screens – Powerful Regressions
Detox is necessary, but it is not enough. Even after several months without screens, if reversed development has not been therapeutically addressed, and if the child has not been guided back toward a typical developmental trajectory with the rebuilding of a functional language system, reintroducing screens can trigger powerful regression. Symptoms return. Perceptual distortions return. Behavioral patterns return (Petrova et al., 2025; Vezenkov & Manolova, 2025b).
Clinically, this is one of the most distressing things to witness. After major gains in regulation, language, eye contact, and daily functioning, just 30 to 60 minutes of songs or videos on a device can undo months of progress and return the child to an autistic-like profile.
That is why the goal is not merely abstinence. The goal is reconstruction: rebuilding attachment, regulation, language, and developmental flexibility so that the old pathway is no longer the child’s fastest route back to safety.
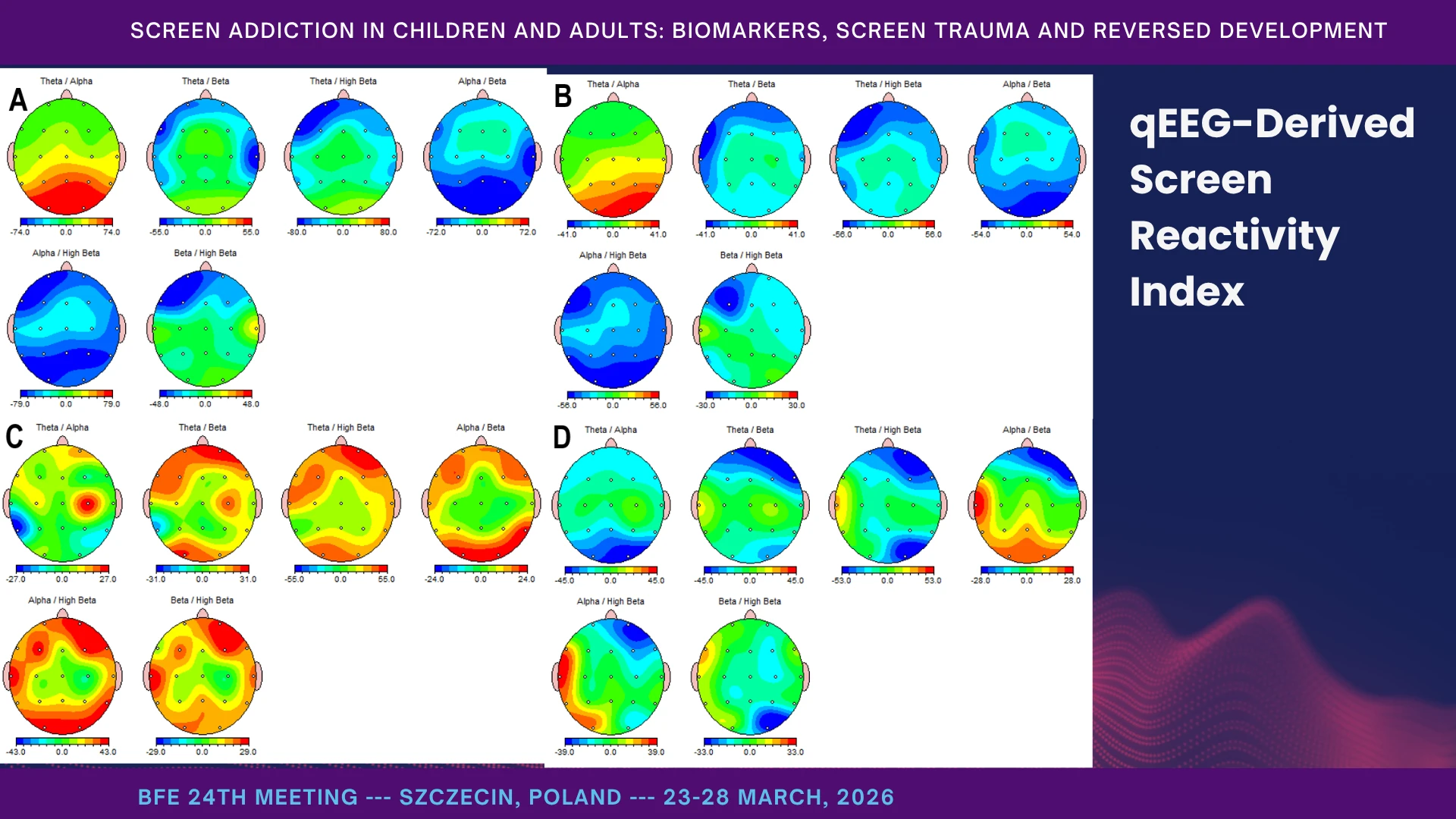
qEEG-Derived Screen Reactivity Index
To move beyond clinical impression, we developed a qEEG-based Screen Reactivity Index. In simple terms, it measures how strongly the brain changes when the child moves from an eyes-open baseline into video viewing.
Before intervention, the deviations were highly state-dependent and became most visible during screen exposure itself. In other words, the screen did not simply reveal a stable abnormality; it actively pulled the brain into a different state. After intervention, the qEEG maps moved closer to normative ranges across conditions, and the extremes of reactivity became less pronounced.
The most striking finding was a biphasic shift in screen reactivity. Before treatment, we often saw what we called a Burnout Response: the screen activated a fatigued, high-theta brain. After treatment, this could invert into what we called a Trance Response: screen exposure now triggered immediate prefrontal slowing or dissociation in a brain that had become more sensitive after detox.
That matters clinically, because it shows two things at once: first, that screen effects are state-dependent and measurable; and second, that recovery does not mean the screen becomes harmless. Often it means the nervous system becomes more visibly reactive to it.
Neurobiology of ASD and ADHD
This is where I state the hypothesis most clearly. In our view, SIPVR, SIPECR, absence of nystagmus, and related functional distortions caused by early screen addiction lie at the core of the pathophysiological mechanisms underlying ASD and related neurodevelopmental disorders such as ADHD, developmental delay, ODD, and others.
The common denominator is vision-dominant processing. When static visual control begins to override vestibular and other sensory functions, sensorimotor integration fragments. Perception narrows. Safety becomes harder to derive from the body, movement, and human co-regulation, and the child begins to organize around danger, rigidity, and repetition.
Reinforcing this mode of functioning effectively legitimizes the ASD diagnosis, whereas reversing it—toward a more human‑specific developmental trajectory—offers a real possibility of full recovery.
In that sense, balance is not merely motor. It is one of the foundations of safe mode. When vestibular function is distorted, the whole sensory field is more easily recruited into chronic alarm: generalized anxiety, freeze, fear, and phylogenetically ancient survival-based behavior. The earlier the exposure to screens, the greater the risk that development will shift toward evolutionarily older and more dysregulated modes of functioning.
This is why the clinical stakes are so high. If we reinforce this mode of functioning, we stabilize the diagnosis. If we reverse it—toward a more human-specific developmental trajectory—we open the possibility of profound recovery.
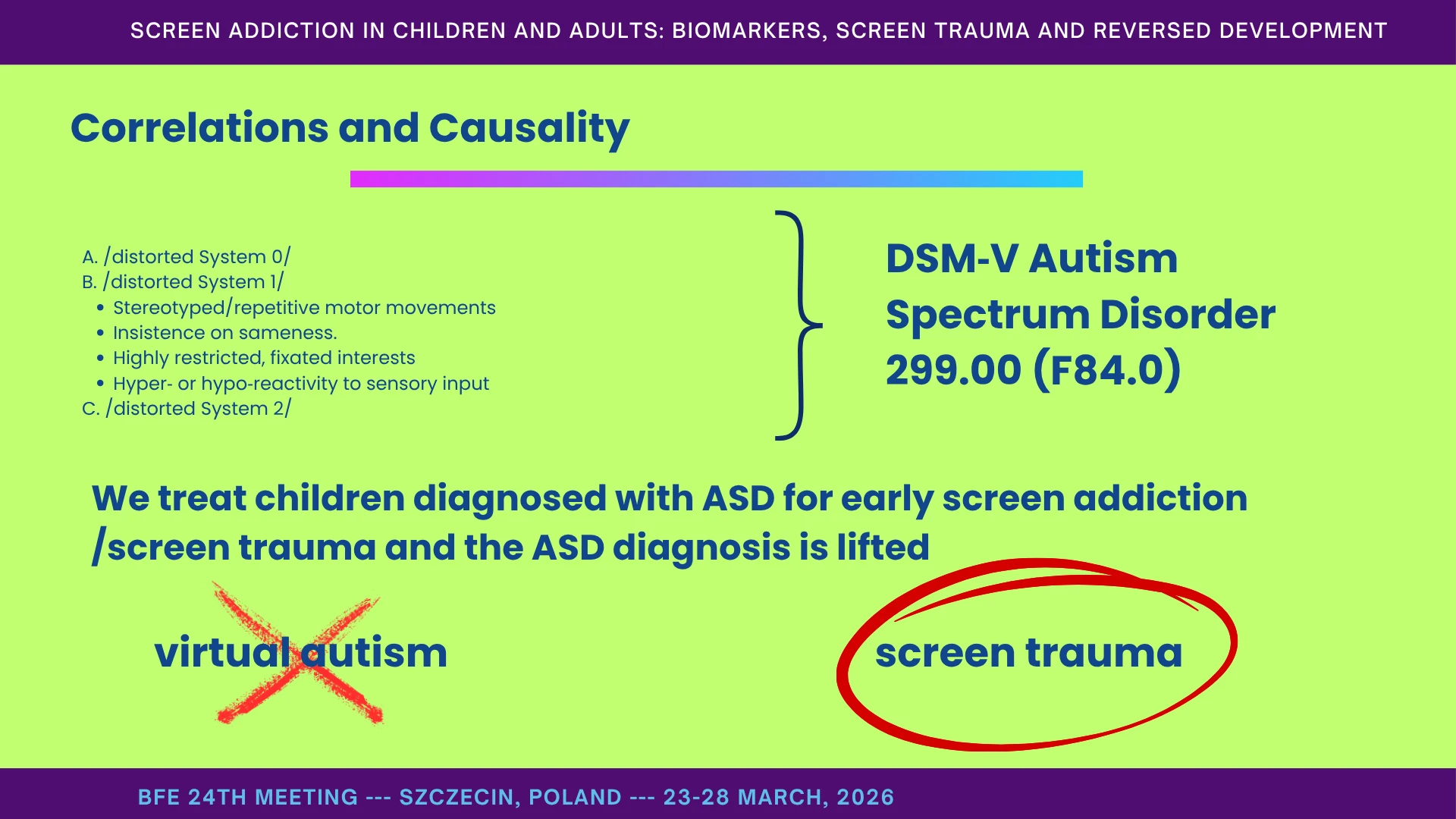
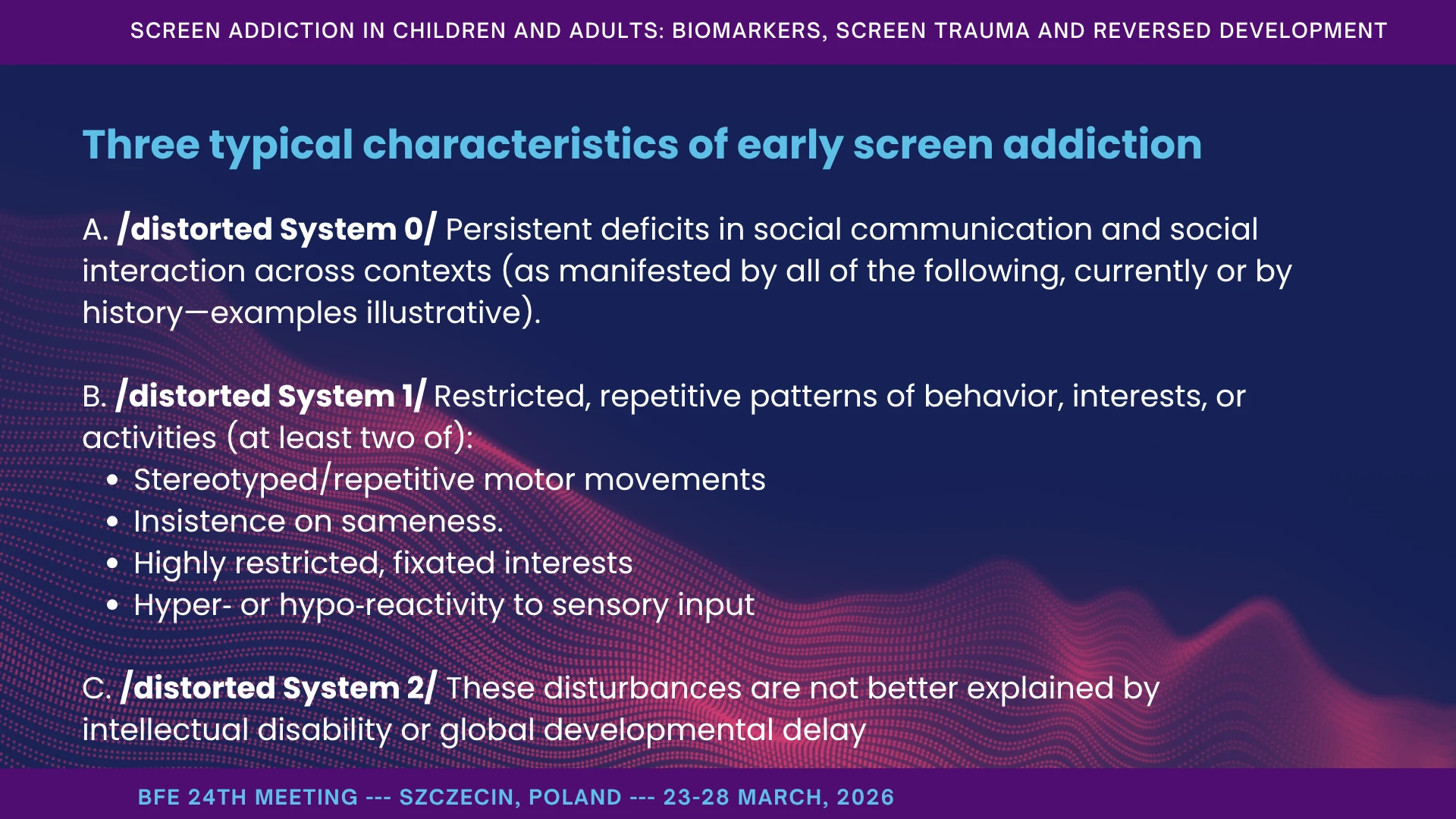
At this point, many of you will recognize something familiar. If we translate our model into clinical language, early screen addiction often presents with three broad clusters: first, distortion of System 0 - failures of social reciprocity, joint attention, and communication across contexts; second, distortion of System 1 - repetitive behavior, ritualization, insistence on sameness, restricted interests, and compulsive sensory patterns; and third, distortion of System 2 - where the picture cannot be fully explained by intellectual disability or global developmental delay alone.
In other words, what I have described functionally maps onto a clinical picture that many people already know from DSM-5 autism spectrum presentations. That is precisely why these children are so often diagnosed as ASD (American Psychiatric Association, n.d.).
This is familiar to some from DSM‑V Autism Spectrum Disorder 299.00 (F84.0).
Clinically, we see two broad patterns. Some children - what has often been called “virtual autism” - improve substantially with screen detox alone. Others do not. In those children, deeper treatment of screen trauma and reversed development is required in 50% of the cases. We treat a child diagnosed with ASD for early screen addiction and screen trauma /reversed development/ and the child no longer meets diagnostic criteria.
Of course, this awaits confirmation via randomized controlled trials with additional control groups.
And one more point is crucial: before attachment to people is restored, and before a real language system is rebuilt, reintroducing screens can trigger powerful regression. That is why the question is not only diagnosis. The question is developmental reversibility (Vezenkov & Manolova, 2025b).
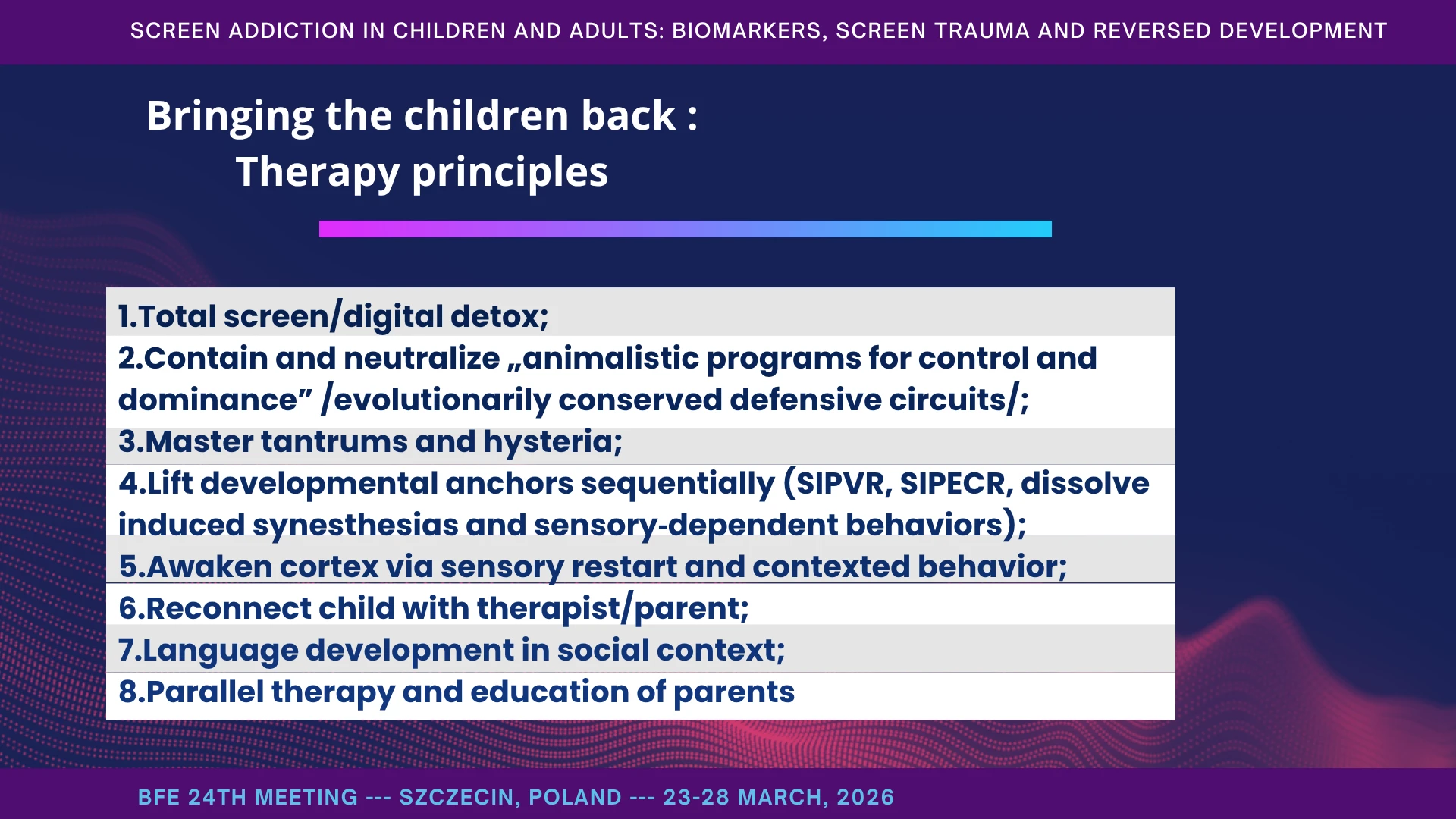
Nootism is not a magical method. It is a practice-derived therapeutic concept for bringing the child back from early screen addiction and screen trauma toward human connectedness and a more typical developmental trajectory.
Its principles are simple, but demanding. First, total screen and digital detox. Second, containment and neutralization of evolutionarily conserved defensive circuits - those patterns of control, dominance, panic, and withdrawal that begin to organize the child’s life. Third, stabilization of tantrums, hysteria, and severe dysregulation.
From there, we work sequentially: lifting developmental anchors such as SIPVR and SIPECR, dissolving induced synesthesia-like loops and sensory-dependent behaviors, awakening the cortex through sensory restart and meaningful behavior in real human context, reconnecting the child with therapist and parent, and rebuilding language in social interaction.
At the same time, parents undergo parallel therapy and education. They must be prepared to reattach to the child and become guides, not service staff for addictive routines. Nootism insists on humanity and empathy for the child - not accommodation of the defensive circuits that hold the child captive. That is also why we reject drill-based behavioral techniques as a primary path.
And finally, Nootism is not only treatment. It also includes prevention: digital hygiene and post-therapy maintenance, for vulnerable patients and for healthy children alike.
Phases of Recovery - Return from Psychotic‑Like Functioning to Full Restoration
Recovery tends to unfold in recognizable phases. We sometimes describe it metaphorically as “returning from the other world.” During full sensory restart, we often speak to the child very directly: “We are here.” “You are here with me.” “Come back to us.”
Often, after the first full restart, we see the first stable eye contact - the first sign that reversed development is beginning to turn. We sometimes call this moment “rebirth”: the child starts to emerge from the intrauterine-like mode and re-enter shared reality.
But this is not a simple upward line. Once the child begins to spend more time “here” than “there,” a period of deep sadness often follows: inconsolable crying, grief-like affect, melancholy. Then comes a different phase - hyperactivity, engagement, interaction, mischief, testing, expansion.
This is also when many parents realize something important: caring for a typically developing child is often harder than caring for a screen-dependent one, because the recovering child is now alive to the world, demanding, exploratory, and relational.
After this hyperactive and disinhibited phase, impulse control gradually begins to appear. Old patterns still alternate with the new, and they are often re-triggered by visual and auditory cues. Recovery, in other words, is real - but it is layered, unstable at first, and deeply state-dependent.
No Child Recovery Without Therapeutic Work with the Parents
Whenever we work therapeutically with a child, we also work therapeutically with the parents. Not merely consultatively, and not merely by giving information. Change comes from the inside out, and for the child it is essential that this change is allowed, encouraged, supported, and met with appropriate feedback by the surrounding adults - by the significant others, by the primary caregivers.
If that does not happen, the child is placed in a painful conflict: between their emerging sense of what is good for them, and the existing family status quo. In other words, the child begins to move toward recovery, while the environment continues to organize around the old system.
So what does it mean to work therapeutically with parents? It means that we do not treat them as observers, but as participants in recovery. We use biofeedback-based neurotherapy, individual sessions, and comprehensive qEEG and ANS assessment when needed, while addressing the parental conditions that block change: depressive and anxiety-related states, unresolved trauma, addictions, and those patterns of functioning that normalize addictions inside the family.
At the same time, we build parental capacity: the ability to support the child’s recovery, to reorganize daily life, to change the emotional climate of the home, and to protect the child from harmful dynamics - including extended family dynamics when necessary.
That is why we draw a clear line: if parents are unwilling to participate actively in the therapeutic process, we decline to work. The child is not an object to be repaired, but a subject in need of profound support. This is a principle on which we do not compromise.
Parents and Caregivers: The Adult Side of Screen Addiction
Therapeutic work with parents is often harder than work with the children themselves. That has become one of our clearest lessons. And yet, for now, it is the only reliable path to effective treatment and durable recovery in the child.
Why is it so difficult? Because the child’s symptoms often exist within a wider family system that is already shaped by anxiety, trauma, addiction, denial, marital disruption, or hidden loyalties. In many cases, the child begins to change, but the environment unconsciously organizes itself to restore the old equilibrium. That is why dropout, relapse, and therapeutic sabotage so often have parental or family-system roots.
Over time, we have described a number of recurring parental patterns in Nootism: parents who are too overwhelmed to sustain change, parents whose own addictions normalize dependence in the family, parents who cannot tolerate the child’s recovery because it destabilizes the household, and parents whose unresolved trauma blocks reattachment.
One of the darkest domains we have encountered involves forms of parental dysfunction in which the child’s symptoms are maintained, amplified, or even unconsciously produced within the caregiving system. In extreme cases, this overlaps with Munchausen syndrome by proxy. In the digital age, this can occur through the repeated use of screens as tools of sedation, control, or symptom production.
That is why parental recovery is not an optional supplement to child therapy. It is one of its central conditions. Without it, the child may improve temporarily, but the family system will often pull development back toward the old state (Manolova et al., 2025; Manolova & Vezenkov, 2025d; Pashina et al., 2025; Petrov et al., 2025).
A Historical-Cultural Theory of Autism’s Recognition and Rising Prevalence
If we look historically at the first countries to introduce autism diagnostics, a striking pattern begins to appear: the recognition of autism tends to follow - sometimes after a few years, sometimes after a generation - the mass penetration of radio, and even more clearly, television. I present this not as final proof, but as a recurring historical pattern that deserves serious attention.
From that perspective, autism can be viewed not only as an individual clinical condition, but also as a neurodevelopmental phenomenon highly sensitive to cultural media environments in early childhood - especially environments that are unidirectional, non-interactive, repetitive, and high in sensory intensity.
Each new wave of screen expansion appears to deepen the pressure: home video and 24-hour children’s channels in the 1980s; portable smart devices, user-generated platforms, and algorithmic short-form video in the 2000s and 2010s; and then the intensified confinement of the COVID period. My argument is that these are not neutral background changes. They progressively reorganize the developmental ecology of childhood.
And now we are entering a new phase. The move from cloud-connected “conversational” dolls to embodied AI agents creates something qualitatively different: a hyper-responsive artificial partner that may displace human co-regulation even more efficiently than passive screens ever did. That is why the next developmental wave may be even more consequential than the previous ones (Manolova & Vezenkov, 2025f).
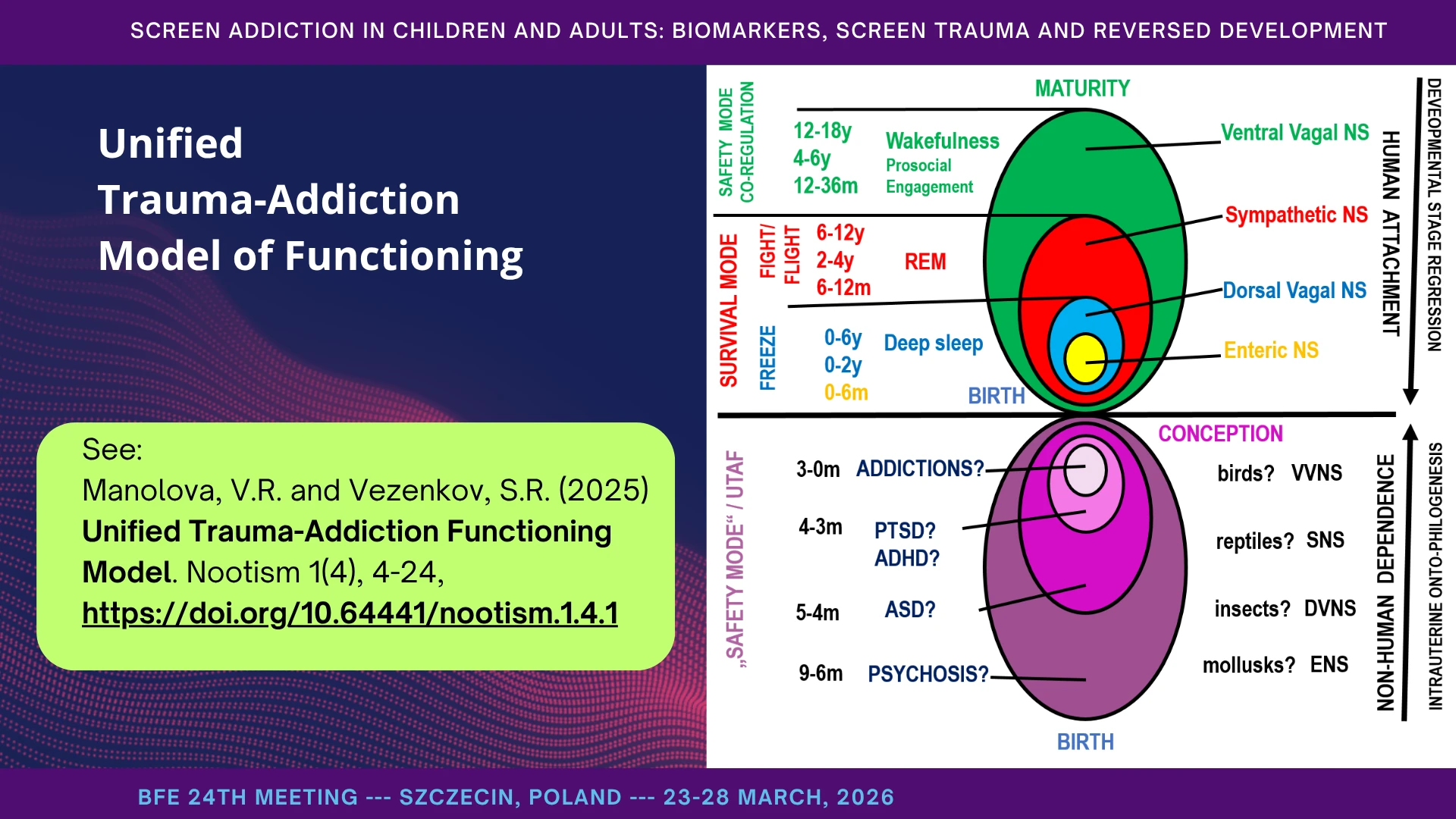
Unified Trauma-Addiction Model of Functioning
To this point I have focused mainly on children. But the same logic extends far beyond childhood. We first developed this model while working with children, yet it applies across the lifespan.
The model begins with a simple but important idea: trauma does not only lead to addiction; addiction itself also generates traumatization. The two processes stabilize one another and form a functional loop. That loop may take the form of one dominant addiction, or several alternating ones - whether substance-based or behavioral.
In that sense, the person becomes dependent not only on a substance, a behavior, or a cue, but on the addiction–trauma mode of functioning itself. The content becomes secondary; the state becomes primary.
That is why substances, cues, and compulsions are merely gateways for re-entry. In adults, the gateway may be alcohol or pornography - but it may also be money, property, power, excessive control, or the compulsive pursuit of conflict. What matters is not the object alone, but the function it serves: rapid return to an older defensive state when higher regulatory systems collapse under overwhelming stress.
And that is how the trauma–addiction loop becomes self-sustaining. It stabilizes, takes hold of the person’s life, and gradually constrains freedom itself (Manolova & Vezenkov, 2025g).
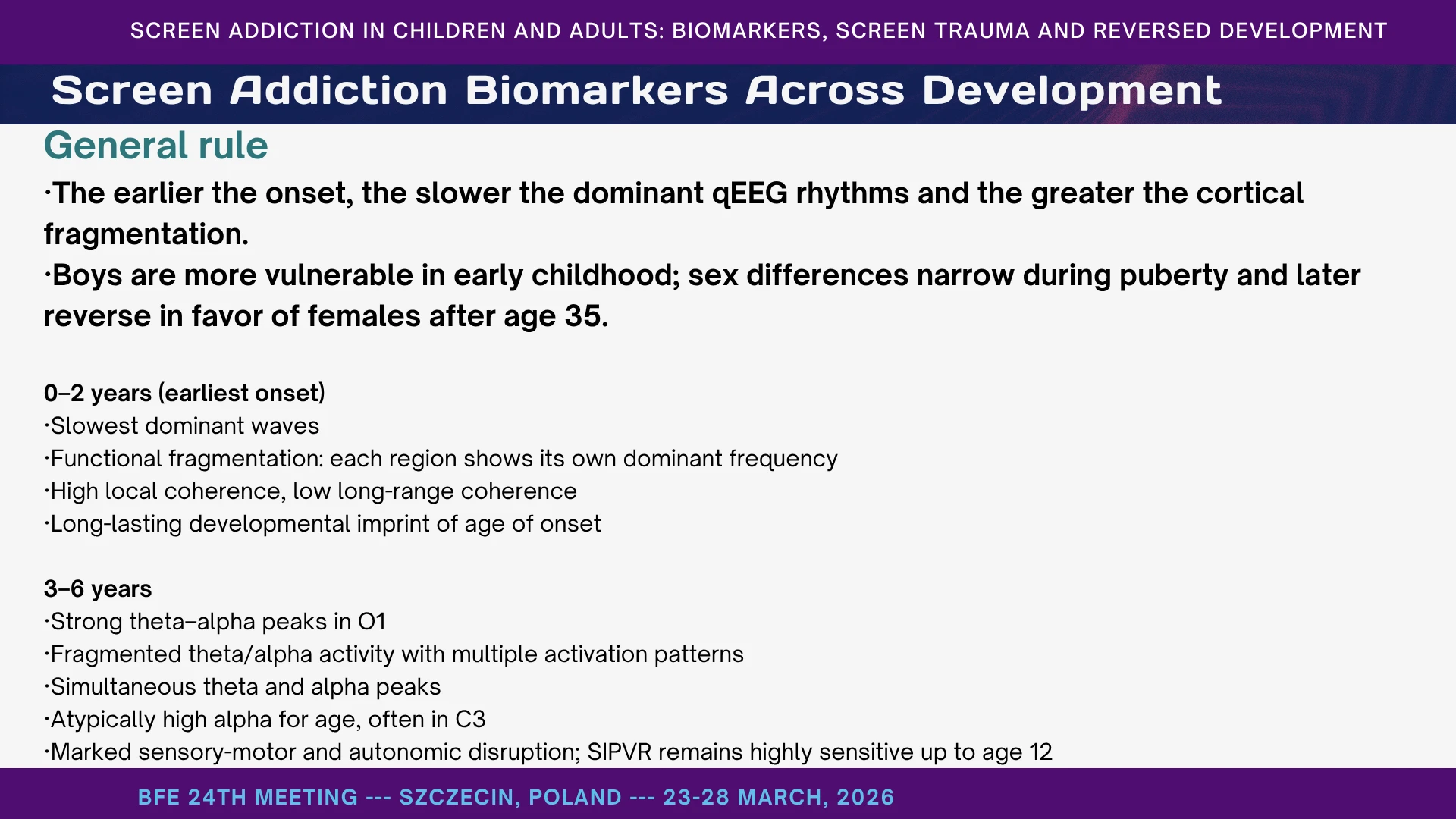
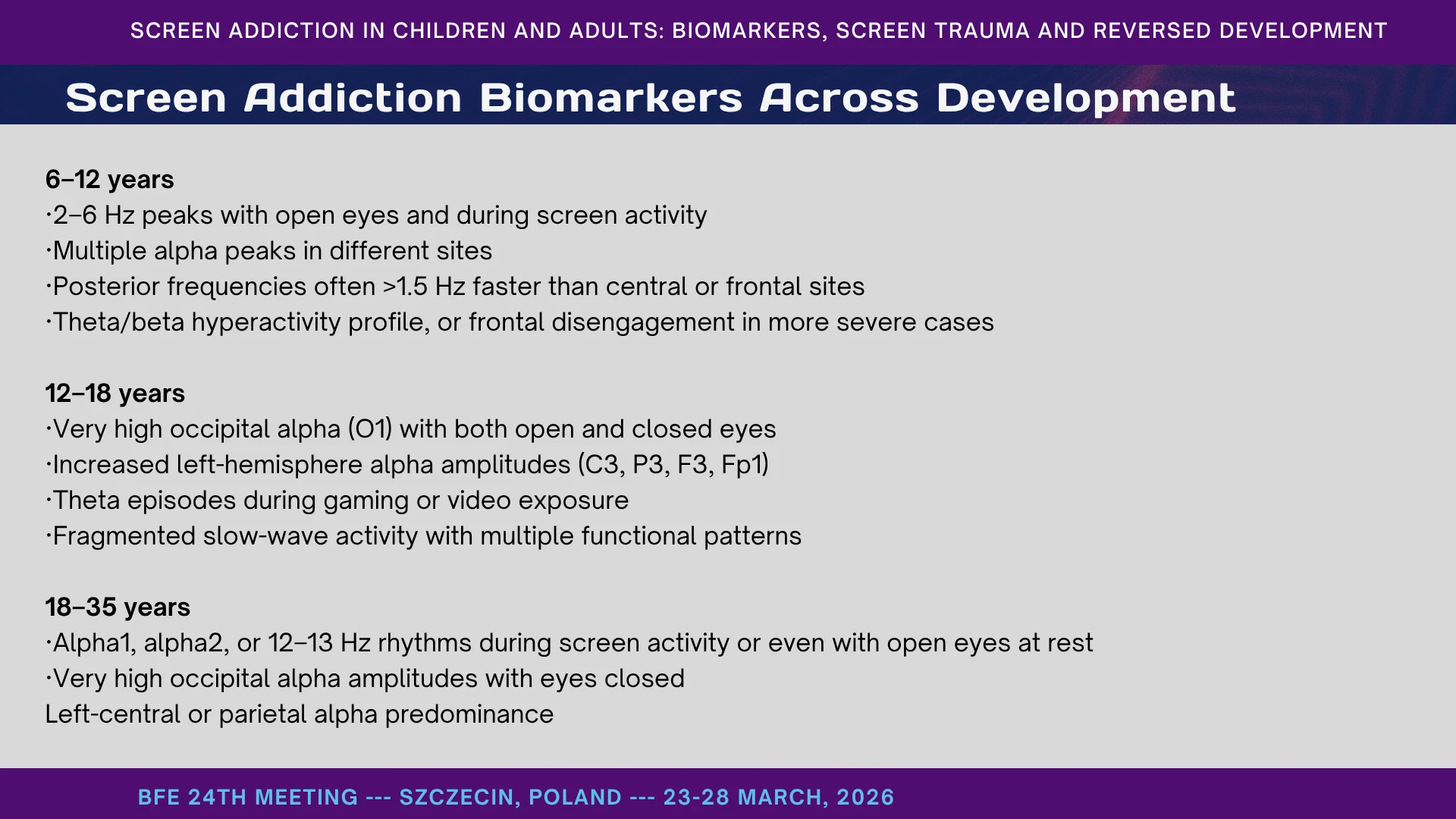
Screen Addiction Biomarkers Across Development
Let us summarize something crucial: screen addiction does not leave the same biomarker profile at every age. The earlier it begins, the slower the dominant rhythms and the more fragmented the cortex becomes. In the youngest children, we see strong slowing, fragmentation, multisite instability, and highly sensitive vestibular markers such as SIPVR. In school-age children, slow-wave peaks and posterior–anterior dissociation remain prominent. In adolescents, very high occipital alpha and left-sided alpha predominance become especially visible. By early adulthood, the pattern shifts toward persistent alpha with open eyes, an overstimulated visual cortex, and growing autonomic imbalance. In other words, screen addiction leaves age-specific neurophysiological signatures across development (Vezenkov & Manolova, 2025c).
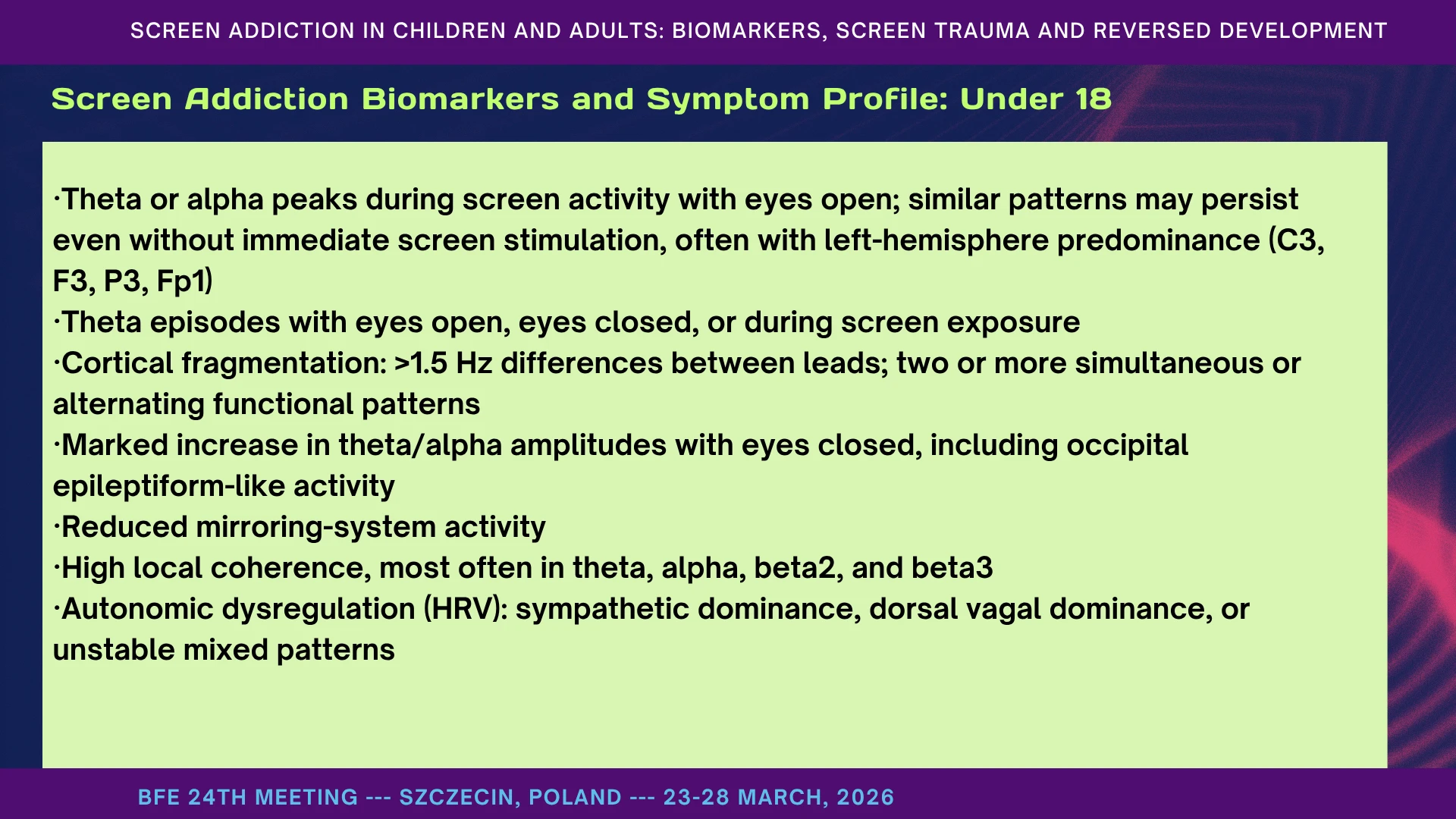
Screen Addiction Biomarkers and Symptom Profile: Under 18
Below the age of 18, the dominant biomarker pattern is slowing with fragmentation. We often see theta or alpha peaks during screen activity with eyes open, and in more affected children the same pattern may persist even without immediate screen exposure. There is marked fragmentation between regions, exaggerated theta–alpha amplitudes with eyes closed, and high local coherence, especially in theta, alpha, and high beta bands. At the same time, HRV shows autonomic dysregulation - sympathetic dominance, dorsal vagal states, or unstable mixed patterns. Clinically, this corresponds to poor concentration, cognitive impatience, anxiety, sleep disruption, and a tendency toward overdiagnosis, because the same child may appear to fit multiple diagnostic labels at once (Aleksandrov et al., 2025; Ivanova et al., 2025; Mateev, Pashina, et al., 2025).
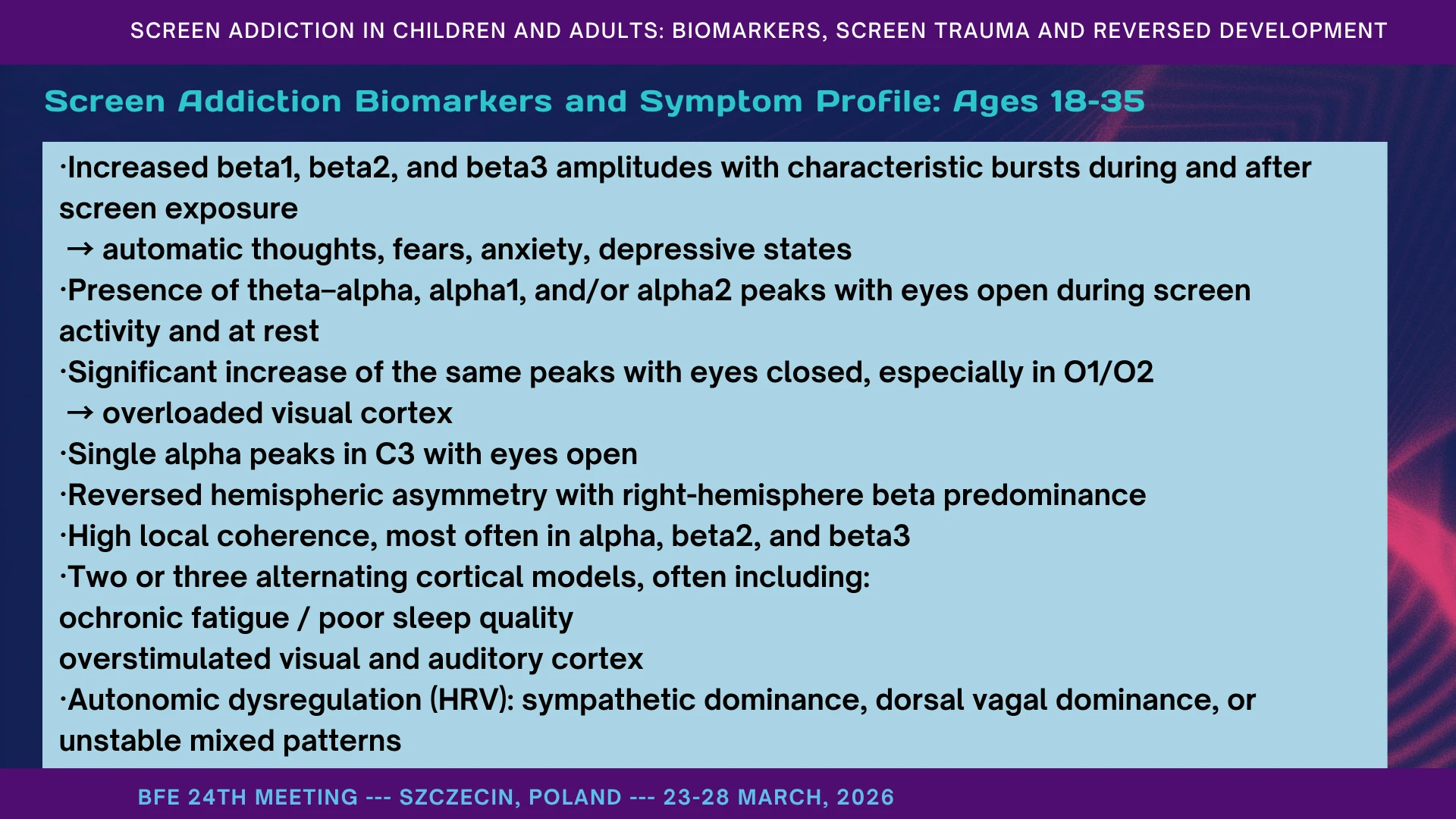
Screen Addiction Biomarkers and Symptom Profile: Ages 18–35
Between 18 and 35, the pattern becomes more mixed: hyperstimulation and exhaustion coexist. We often see bursts in beta1, beta2, and beta3 during and after screen exposure, together with theta–alpha and alpha peaks that persist even with eyes open. With eyes closed, these peaks often increase sharply, especially in O1 and O2, suggesting an overloaded visual cortex. High local coherence remains common, but we often see two or three alternating cortical modes in the same person: one dominated by fatigue and poor sleep, another by visual and auditory overstimulation. HRV again shows unstable autonomic regulation. Clinically, this age group often presents with panic, anxiety, headaches, chronic fatigue, burnout, irritability, muscle tension, IBS, and sexual dysfunction - signs that the screen has become both a source of stress and a failed method of self-regulation (Alexandrov et al., 2025; Manolova & Vezenkov, 2025c).
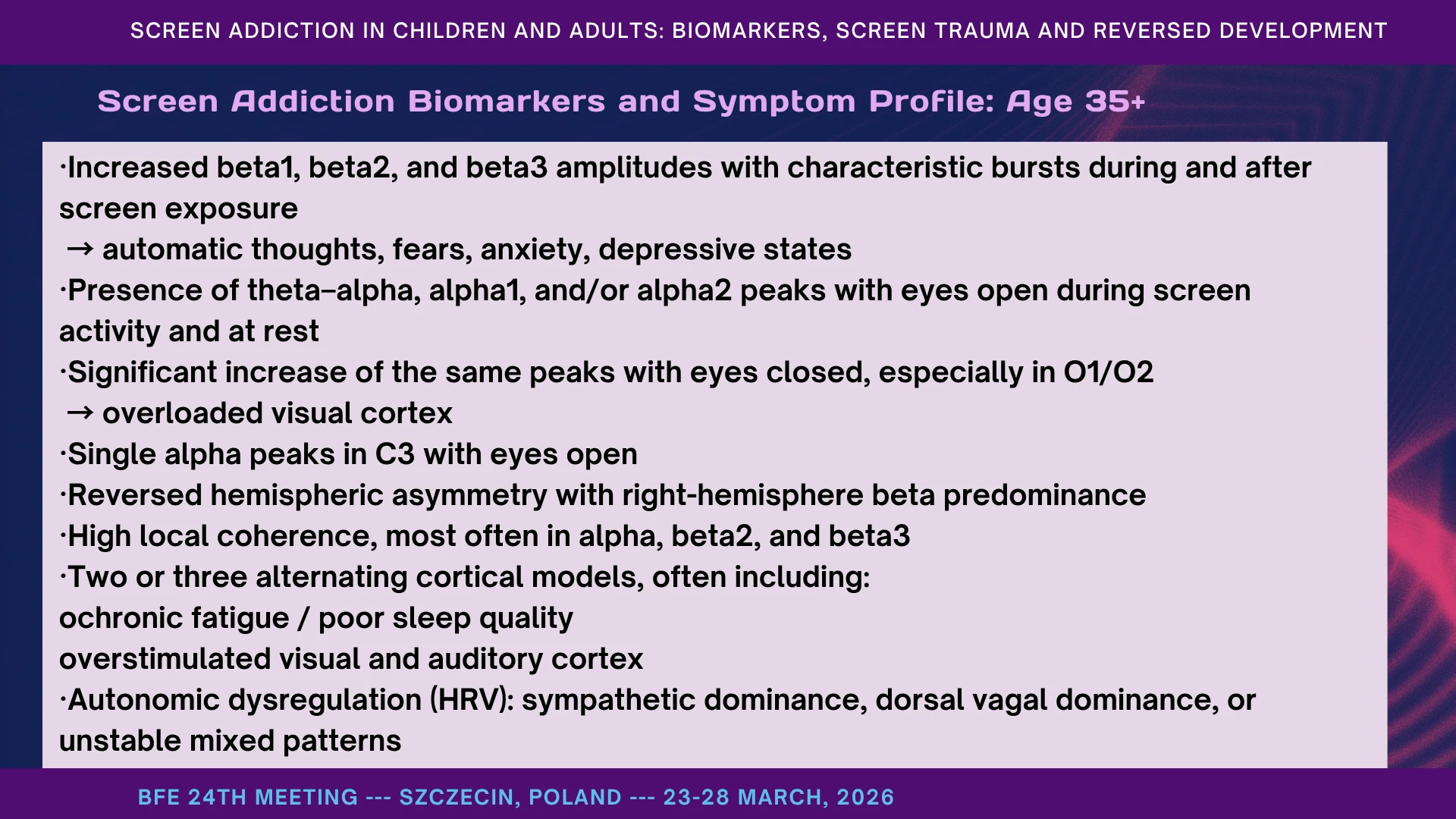
Screen Addiction Biomarkers and Symptom Profile: Age 35+
After 35, the pattern often shifts from overt overstimulation toward chronic dysregulation and cognitive decline. Beta bursts remain common during and after screen exposure, but what becomes especially striking is the lack of normal alpha blocking with eyes closed - the classic busy-brain picture, often accompanied by poor sleep and mental exhaustion. Right-hemisphere beta predominance and high local coherence persist, and HRV continues to show unstable autonomic balance. Clinically, these patients may present not only with anxiety, depression, and burnout, but also with difficulty thinking clearly, reduced tolerance for complexity, withdrawal from intellectually demanding work, rigid fixations, automatic behaviors, and in some cases a drift toward fantasy, illusion, or conspiratorial thinking in place of disciplined thought (Manolova & Vezenkov, 2025c, 2025b; Pashina et al., 2025).
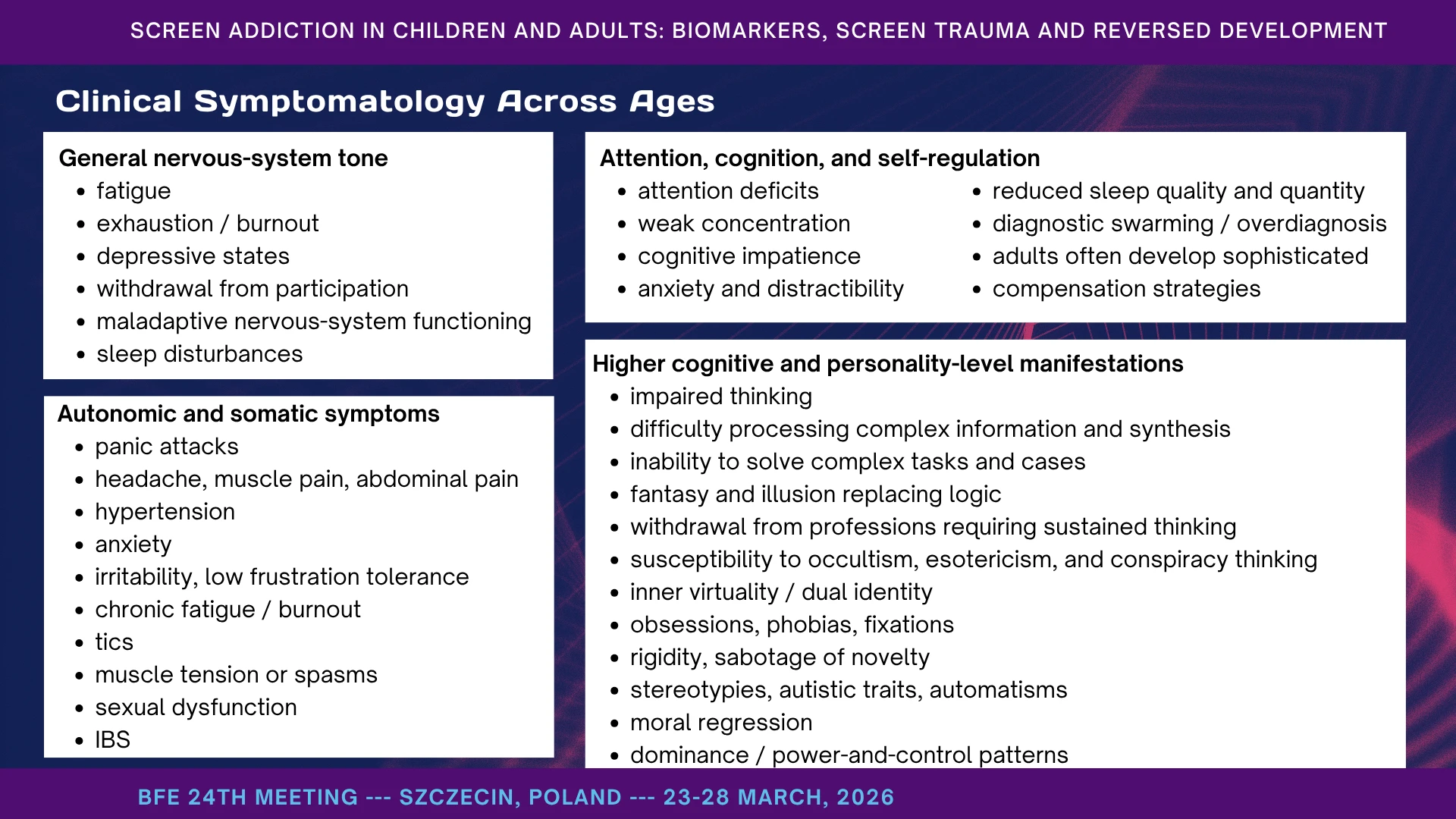
Clinical Symptomatology Across Ages
When these biomarker patterns become clinically embodied, they appear as a broad syndrome of dysregulation. At the level of general nervous-system tone, we see fatigue, exhaustion, depressive states, sleep disturbance, withdrawal, and a chronic sense that the system is no longer adapting well. At the autonomic and somatic level, the picture includes panic attacks, headaches, muscle and abdominal pain, hypertension, anxiety, irritability, tics, chronic fatigue, burnout, sexual dysfunction, and IBS. Cognitively, the pattern is equally striking: weak concentration, attentional instability, cognitive impatience, distractibility, reduced sleep quality, and in many cases a kind of diagnostic swarming, where the same person seems to accumulate multiple labels at once. Adults often compensate cleverly, which is why the dysfunction may remain hidden for years. At the highest levels, the damage becomes existential: thinking becomes harder, complexity becomes intolerable, fantasy begins to replace logic, and the person becomes more vulnerable to fixations, rigidity, automatisms, and power-and-control patterns. In that sense, screen addiction is not merely a habit. It is a condition that can reshape body, mind, character, and freedom.
Clinical Conclusions: Source, Amplifier, and Possibility of Recovery
The conclusion is simple, even if the implications are not. Screen addiction is both a source and an amplifier of dysfunction. It can aggravate what is already present, unmask what is latent, and generate entirely new patterns of symptom escalation and collapse. That is why it changes the effectiveness of virtually any therapy - medical, psychological, biofeedback, EEG neurofeedback, or educational. But there is a second conclusion, and this is the one I want to emphasize most strongly: these disturbances are functional. That means they are reversible, modifiable, and treatable. In many cases, they are compatible with profound recovery, and sometimes even with full restoration of development and functioning. This does not mean recovery is easy. In some patients, early developmental anchors remain, and detox alone is not enough. But it does mean something essential: we are not dealing only with fixed damage. We are dealing with living systems that can still change. And that is why this work matters - not only to diagnose suffering, but to reopen the path toward freedom, development, and human life.

Instead of a Conclusion: One Message
You do not have to agree with every hypothesis I have presented today. But if you remember only one thing, let it be this: a young child learns from people, not from screens.
If we give the child back the human world - face, voice, touch, rhythm, waiting, language, and love - development can begin to turn again. That is our hope. That is our work. And that is why this is not a war against technology. It is a defense of the human being.
We may continue to build smarter machines. The real question is whether we will still raise human children. Because no screen, no algorithm, no robot can replace the living presence through which a child becomes a self.
Technology can be a tool. It must never become the child’s world.
Let us awaken - because the human being becomes fully human only in wakeful relation to another human.
Let us give our children back the human world!..
Refrences
Al-Beltagi, M. (2024). Nutritional management and autism spectrum disorder: A systematic review. World Journal of Clinical Pediatrics, 13(4), 99649. https://doi.org/10.5409/wjcp.v13.i4.99649
Aleksandrov, I., Manolova, V. R., & Vezenkov, S. R. (2025). Integrative Biofeedback Therapy in a Treatment-Resistant Schizophrenia Case with Screen Addiction: Insights from qEEG and HRV. Nootism, 1(4), 25–37. https://doi.org/10.64441/nootism.1.4.2
Alexandrov, I., Manolova, V., & Vezenkov, S. (2025). Infantile Behavior Patterns and Developmental Delays in Adolescents and Young Adults (Aged 12-29) with Screen Addiction. Nootism, 1(1), 79–82. https://doi.org/10.64441/nootism.2NCSC.8
American Psychiatric Association. (n.d.). Diagnostic and Statistical Manual of Mental Disorders | Psychiatry Online. DSM Library. Retrieved January 11, 2026, from https://psychiatryonline.org/doi/book/10.1176/appi.books.9780890425596
Anderson, D. R., & Pempek, T. A. (2005). Television and Very Young Children. American Behavioral Scientist, 48(5), 505–522. https://doi.org/10.1177/0002764204271506
Arnsten, A. F. T. (2009). Stress signalling pathways that impair prefrontal cortex structure and function. Nature Reviews Neuroscience, 10(6), 410–422. https://doi.org/10.1038/nrn2648
Aureli, T., Presaghi, F., & Garito, M. C. (2022). Mother-infant co-regulation during infancy: Developmental changes and influencing factors. Infant Behavior & Development, 69, 101768. https://doi.org/10.1016/j.infbeh.2022.101768
Baron-Cohen, S., Ashwin, E., Ashwin, C., Tavassoli, T., & Chakrabarti, B. (2009). Talent in autism: Hyper-systemizing, hyper-attention to detail and sensory hypersensitivity. Philosophical Transactions of the Royal Society B: Biological Sciences, 364(1522), 1377–1383. https://doi.org/10.1098/rstb.2008.0337
Bellato, A., Arora, I., Kochhar, P., Ropar, D., Hollis, C., & Groom, M. J. (2022). Heart Rate Variability in Children and Adolescents with Autism, ADHD and Co-occurring Autism and ADHD, During Passive and Active Experimental Conditions. Journal of Autism and Developmental Disorders, 52(11), 4679–4691. https://doi.org/10.1007/s10803-021-05244-w
Bird, S., Moid, L. A. E., Jones, C. A., & Surtees, A. D. R. (2024). The relationships between restrictive/repetitive behaviours, intolerance of uncertainty, and anxiety in autism: A systematic review and meta-analysis. Research in Autism Spectrum Disorders, 117, 102428. https://doi.org/10.1016/j.rasd.2024.102428
Birulés, J., Goupil, L., Josse, J., & Fort, M. (2023). The Role of Talking Faces in Infant Language Learning: Mind the Gap between Screen-Based Settings and Real-Life Communicative Interactions. Brain Sciences, 13(8), 1167. https://doi.org/10.3390/brainsci13081167
Blum, K., Baron, D., Lott, L., Ponce, J. V., Siwicki, D., Boyett, B., Steinberg, B., Modestino, E. J., Fried, L., Hauser, M., Simpatico, T., Downs, B. W., McLaughlin, T., Hajela, R., & Badgaiyan, R. D. (2020). In Search of Reward Deficiency Syndrome (RDS)-Free Controls: The “Holy Grail” in Genetic Addiction Risk Testing. Current Psychopharmacology, 9(1), 7–21. https://doi.org/10.2174/2211556008666191111103152
Blum, K., Braverman, E. R., Holder, J. M., Lubar, J. F., Monastra, V. J., Miller, D., Lubar, J. O., Chen, T. J. H., & Comings, D. E. (2000). The Reward Deficiency Syndrome: A Biogenetic Model for the Diagnosis and Treatment of Impulsive, Addictive and Compulsive Behaviors. Journal of Psychoactive Drugs, 32(sup1), 1–112. https://doi.org/10.1080/02791072.2000.10736099
Bornstein, M. H., & Esposito, G. (2023). Coregulation: A Multilevel Approach via Biology and Behavior. Children, 10(8), 1323. https://doi.org/10.3390/children10081323
Bottema‐Beutel, K. (2016). Associations between joint attention and language in autism spectrum disorder and typical development: A systematic review and meta‐regression analysis. Autism Research, 9(10), 1021–1035. https://doi.org/10.1002/aur.1624
Brushe, M. E., Haag, D. G., Melhuish, E. C., Reilly, S., & Gregory, T. (2024). Screen Time and Parent-Child Talk When Children Are Aged 12 to 36 Months. JAMA Pediatrics, 178(4), 369. https://doi.org/10.1001/jamapediatrics.2023.6790
Cahalan, S., Mitroff, S. R., Subiaul, F., & Rosenblau, G. (2025). Using the cognitive rigidity-flexibility dimension to deepen our understanding of the autism spectrum. Personality Neuroscience, 8, e3. https://doi.org/10.1017/pen.2025.10002
Chen, J.-Y., Strodl, E., Huang, L.-H., Chen, Y.-J., Yang, G.-Y., & Chen, W.-Q. (2020). Early Electronic Screen Exposure and Autistic-Like Behaviors among Preschoolers: The Mediating Role of Caregiver-Child Interaction, Sleep Duration and Outdoor Activities. Children, 7(11), 200. https://doi.org/10.3390/children7110200
Chisari, D., Vitkovic, J., Clark, R., & Rance, G. (2024a). Vestibular Function and Postural Control in Children with Autism Spectrum Disorder. Journal of Clinical Medicine, 13(17), 5323. https://doi.org/10.3390/jcm13175323
Chisari, D., Vitkovic, J., Clark, R., & Rance, G. (2024b). Vestibular Function and Postural Control in Children with Autism Spectrum Disorder. Journal of Clinical Medicine, 13(17), 5323. https://doi.org/10.3390/jcm13175323
Chung, S., & Son, J.-W. (2020). Visual Perception in Autism Spectrum Disorder: A Review of Neuroimaging Studies. Journal of the Korean Academy of Child and Adolescent Psychiatry, 31(3), 105–120. https://doi.org/10.5765/jkacap.200018
Conboy, B. T., Brooks, R., Meltzoff, A. N., & Kuhl, P. K. (2015). Social Interaction in Infants’ Learning of Second-Language Phonetics: An Exploration of Brain-Behavior Relations. Developmental Neuropsychology, 40(4), 216–229. https://doi.org/10.1080/87565641.2015.1014487
Coyne, S. M., Reschke, P. J., Stockdale, L., Gale, M., Shawcroft, J., Gentile, D. A., Brown, M., Ashby, S., Siufanua, M., & Ober, M. (2023). Silencing screaming with screens: The longitudinal relationship between media emotion regulation processes and children’s emotional reactivity, emotional knowledge, and empathy. Emotion, 23(8), 2194–2204. https://doi.org/10.1037/emo0001222
Dapretto, M., Davies, M. S., Pfeifer, J. H., Scott, A. A., Sigman, M., Bookheimer, S. Y., & Iacoboni, M. (2006). Understanding emotions in others: Mirror neuron dysfunction in children with autism spectrum disorders. Nature Neuroscience, 9(1), 28–30. https://doi.org/10.1038/nn1611
Davis, M., Bilms, J., & Suveg, C. (2017). In Sync and in Control: A Meta-Analysis of Parent-Child Positive Behavioral Synchrony and Youth Self-Regulation. Family Process, 56(4), 962–980. https://doi.org/10.1111/famp.12259
de Faria, O., Pivonkova, H., Varga, B., Timmler, S., Evans, K. A., & Káradóttir, R. T. (2021). Periods of synchronized myelin changes shape brain function and plasticity. Nature Neuroscience, 24(11), 1508–1521. https://doi.org/10.1038/s41593-021-00917-2
Dresp-Langley, B. (2020a). Children’s Health in the Digital Age (No. 2020030258). Preprints. https://doi.org/10.20944/preprints202003.0258.v1
Dresp-Langley, B. (2020b). Children’s Health in the Digital Age (No. 2020030258). Preprints. https://doi.org/10.20944/preprints202003.0258.v1
Feldman, J. I., Dunham, K., Cassidy, M., Wallace, M. T., Liu, Y., & Woynaroski, T. G. (2018). Audiovisual multisensory integration in individuals with autism spectrum disorder: A systematic review and meta-analysis. Neuroscience & Biobehavioral Reviews, 95, 220–234. https://doi.org/10.1016/j.neubiorev.2018.09.020
Forest, T. A., McCormick, S. A., Davel, L., Mlandu, N., Zieff, M. R., Khula South Africa Data Collection Team, Amso, D., Donald, K. A., & Gabard-Durnam, L. J. (2025). Early Caregiver Predictability Shapes Neural Indices of Statistical Learning Later in Infancy. Developmental Science, 28(1), e13570. https://doi.org/10.1111/desc.13570
Friston, K. (2010). The free-energy principle: A unified brain theory? Nature Reviews Neuroscience, 11(2), 127–138. https://doi.org/10.1038/nrn2787
Galaj, E., & Xi, Z.-X. (2021). Progress in opioid reward research: From a canonical two-neuron hypothesis to two neural circuits. Pharmacology Biochemistry and Behavior, 200, 173072. https://doi.org/10.1016/j.pbb.2020.173072
Galli, J., Dusi, L., Garofalo, G., Brizzi, A., Gritti, M., Polo, F., Fazzi, E., & Buccino, G. (2025). Children with autistic spectrum disorder can imagine actions - What can this reveal about the Broken Mirror Hypothesis? Frontiers in Neurology, 16, 1490445. https://doi.org/10.3389/fneur.2025.1490445
Hamilton, A. F. de C. (2013a). Reflecting on the mirror neuron system in autism: A systematic review of current theories. Developmental Cognitive Neuroscience, 3, 91–105. https://doi.org/10.1016/j.dcn.2012.09.008
Hamilton, A. F. de C. (2013b). Reflecting on the mirror neuron system in autism: A systematic review of current theories. Developmental Cognitive Neuroscience, 3, 91–105. https://doi.org/10.1016/j.dcn.2012.09.008
Happé, F., & Frith, U. (2006). The Weak Coherence Account: Detail-focused Cognitive Style in Autism Spectrum Disorders. Journal of Autism and Developmental Disorders, 36(1), 5–25. https://doi.org/10.1007/s10803-005-0039-0
Huttenlocher, P. R. (1984). Synapse elimination and plasticity in developing human cerebral cortex. American Journal of Mental Deficiency, 88(5), 488–496.
Hutton, J. S., Dudley, J., Horowitz-Kraus, T., DeWitt, T., & Holland, S. K. (2020). Associations Between Screen-Based Media Use and Brain White Matter Integrity in Preschool-Aged Children. JAMA Pediatrics, 174(1), e193869. https://doi.org/10.1001/jamapediatrics.2019.3869
Iacoboni, M., & Dapretto, M. (2006). The mirror neuron system and the consequences of its dysfunction. Nature Reviews Neuroscience, 7(12), 942–951. https://doi.org/10.1038/nrn2024
Ivanova, V., Mitsova, S., Petrova, T., Manolova, V., & Vezenkov, S. (2025). Full Recovery of a 10-Year-Old Girl with Persistent Screen Addiction Since Age 2 and Autism Spectrum Disorder: Case Report. Nootism, 1, 17–26. https://doi.org/10.64441/nootism.1.3.3
Jackson, J. H. (1884). The Croonian Lectures on Evolution and Dissolution of the Nervous System. British Medical Journal, 1(1215), 703–707. https://doi.org/10.1136/bmj.1.1215.703
Just, M. A. (2004). Cortical activation and synchronization during sentence comprehension in high-functioning autism: Evidence of underconnectivity. Brain, 127(8), 1811–1821. https://doi.org/10.1093/brain/awh199
Kahneman, D. (2011). Thinking, fast and slow. Farrar, Straus and Giroux. New York.
Kahneman, D., & Tversky, A. (1984). Choices, values, and frames. American Psychologist, 39(4), 341–350. https://doi.org/10.1037/0003-066X.39.4.341
Koob, G. F., & Volkow, N. D. (2016). Neurobiology of addiction: A neurocircuitry analysis. The Lancet Psychiatry, 3(8), 760–773. https://doi.org/10.1016/S2215-0366(16)00104-8
Kuhl, P. K., Tsao, F.-M., & Liu, H.-M. (2003). Foreign-language experience in infancy: Effects of short-term exposure and social interaction on phonetic learning. Proceedings of the National Academy of Sciences, 100(15), 9096–9101. https://doi.org/10.1073/pnas.1532872100
Lage, C., Smith, E. S., & Lawson, R. P. (2024). A meta-analysis of cognitive flexibility in autism spectrum disorder. Neuroscience & Biobehavioral Reviews, 157, 105511. https://doi.org/10.1016/j.neubiorev.2023.105511
León Méndez, M., Padrón, I., Fumero, A., & Marrero, R. J. (2024). Effects of internet and smartphone addiction on cognitive control in adolescents and young adults: A systematic review of fMRI studies. Neuroscience and Biobehavioral Reviews, 159, 105572. https://doi.org/10.1016/j.neubiorev.2024.105572
Lillard, A. S., & Peterson, J. (2011). The Immediate Impact of Different Types of Television on Young Children’s Executive Function. Pediatrics, 128(4), 644–649. https://doi.org/10.1542/peds.2010-1919
Lin, I.-M., & Peper, E. (2009). Psychophysiological Patterns During Cell Phone Text Messaging: A Preliminary Study. Applied Psychophysiology and Biofeedback, 34(1), 53–57. https://doi.org/10.1007/s10484-009-9078-1
Madigan, S., Browne, D., Racine, N., Mori, C., & Tough, S. (2019). Association Between Screen Time and Children’s Performance on a Developmental Screening Test. JAMA Pediatrics, 173(3), 244. https://doi.org/10.1001/jamapediatrics.2018.5056
Maia, T. V., & Frank, M. J. (2011). From reinforcement learning models to psychiatric and neurological disorders. Nature Neuroscience, 14(2), 154–162. https://doi.org/10.1038/nn.2723
Mallawaarachchi, S., Burley, J., Mavilidi, M., Howard, S. J., Straker, L., Kervin, L., Staton, S., Hayes, N., Machell, A., Torjinski, M., Brady, B., Thomas, G., Horwood, S., White, S. L. J., Zabatiero, J., Rivera, C., & Cliff, D. (2024). Early Childhood Screen Use Contexts and Cognitive and Psychosocial Outcomes: A Systematic Review and Meta-analysis. JAMA Pediatrics, 178(10), 1017–1026. https://doi.org/10.1001/jamapediatrics.2024.2620
Manolova, V., Pashina, I., Mateev, M., & Vezenkov, S. (2025). Munchausen Syndrome by Proxy and Other Forms of Parental Abuse in Children with Screen Addiction and a Diagnosis of Autism (ASD) and/or ADHD. Nootism, 1(2), 11–30. https://doi.org/10.64441/nootism.1.2.2
Manolova, V., & Vezenkov, S. (2025a). Are Screen-Induced Synesthesia and Screen-induced Cue-Dependent Behavior Contributing Factors in the Misdiagnosis of ASD Among Children with Screen Addiction? Nootism, 1, 11–16. https://doi.org/10.64441/nootism.1.3.2
Manolova, V., & Vezenkov, S. (2025b). Chronic Intimate Partner Violence, Autonomic Dysregulation, and Intergenerational Impact: A Case Study with HRV Analysis. Nootism, 1(5), 35–43. https://doi.org/10.64441/nootism.1.5.3
Manolova, V., & Vezenkov, S. (2025c). Cortico-Autonomic Dysregulation in Generalized Anxiety Disorder and Irritable Bowel Syndrome: A Combined EEG–HRV Case Study. Nootism, 1(5), 21–34. https://doi.org/10.64441/nootism.1.5.2
Manolova, V., & Vezenkov, S. (2025d). Parental Models: A Profile of the Dynamics in Children Dropping Out of Therapy Programs for Screen Addiction. Nootism, 1(1), 96–100. https://doi.org/10.64441/nootism.2NCSC.11
Manolova, V., & Vezenkov, S. (2025e). Screen Trauma – Specifics of the Disorder and Therapy in Adults and Children. Nootism, 1(1), 37–51. https://doi.org/10.64441/nootism.2NCSC.3
Manolova, V., & Vezenkov, S. (2025f). Screen-Mediated Developmental Deviation: A Historical-Cultural Theory of Autism’s Recognition and Rising Prevalence. Nootism, 1(6), 31–43. https://doi.org/10.64441/nootism.1.6.3
Manolova, V., & Vezenkov, S. (2025g). Unified Trauma-Addiction Functioning Model. Nootism, 1(4), 4–24. https://doi.org/10.64441/nootism.1.4.1
Mateev, M., Manolova, V., & Vezenkov, S. (2025). From Nonverbal to Language – How to Counteract Anti-Human Programming Controlling Children with Early Screen Addiction. Nootism, 1(1), 52–58. https://doi.org/10.64441/nootism.2NCSC.4
Mateev, M., Pashina, I., Manolova, V., & Vezenkov, S. (2025). Restoring Neural Coherence Through Screen Addiction Therapy in a 12-Year-Old with Autism Spectrum Disorder: A Case Report. Nootism, 1, 27–33. https://doi.org/10.64441/nootism.1.3.4
Mathiak, K., & Weber, R. (2006). Toward brain correlates of natural behavior: fMRI during violent video games. Human Brain Mapping, 27(12), 948–956. https://doi.org/10.1002/hbm.20234
McDaniel, B. T., Ventura, A. K., Coyne, S. M., Wolfers, L. N., Pfafman, R., Shinde, A. S., Uva, S., Coleman, B., Ceja Almontes, K. I., & Galovan, A. M. (2026). Crying, Cradles, and Cellphones: A Longitudinal Examination of Infant Media Emotion Regulation and Socio-Emotional Development in Early Infancy. Infancy, 31(1), e70069. https://doi.org/10.1111/infa.70069
Mercure, E., Kushnerenko, E., Goldberg, L., Bowden-Howl, H., Coulson, K., Johnson, M. H., & MacSweeney, M. (2019). Language experience influences audiovisual speech integration in unimodal and bimodal bilingual infants. Developmental Science, 22(1), e12701. https://doi.org/10.1111/desc.12701
Mink, J. W. (1996). THE BASAL GANGLIA: FOCUSED SELECTION AND INHIBITION OF COMPETING MOTOR PROGRAMS. Progress in Neurobiology, 50(4), 381–425. https://doi.org/10.1016/S0301-0082(96)00042-1
Mundy, P., & Newell, L. (2007). Attention, Joint Attention, and Social Cognition. Current Directions in Psychological Science, 16(5), 269–274. https://doi.org/10.1111/j.1467-8721.2007.00518.x
Neo, W. S., Foti, D., Keehn, B., & Kelleher, B. (2023). Resting-state EEG power differences in autism spectrum disorder: A systematic review and meta-analysis. Translational Psychiatry, 13(1), 389. https://doi.org/10.1038/s41398-023-02681-2
Ornitz, E. M. (1974). Effect of Visual Input on Vestibular Nystagmus in Autistic Children. Archives of General Psychiatry, 31(3), 369. https://doi.org/10.1001/archpsyc.1974.01760150075011
Panksepp, J. (1979). A neurochemical theory of autism. Trends in Neurosciences, 2, 174–177. https://doi.org/10.1016/0166-2236(79)90071-7
Pashina, I., Manolova, V., & Vezenkov, S. (2025). Parental Recovery as a Key Factor for the Recovery of Children with Screen Addiction – Biofeedback Therapy for Severe Disorders. Nootism, 1(1), 83–89. https://doi.org/10.64441/nootism.2NCSC.9
Pastor-Cerezuela, G., Fernández-Andrés, M.-I., Sanz-Cervera, P., & Marín-Suelves, D. (2020). The impact of sensory processing on executive and cognitive functions in children with autism spectrum disorder in the school context. Research in Developmental Disabilities, 96, 103540. https://doi.org/10.1016/j.ridd.2019.103540
Peper, E., & Harvey, R. (2018). Digital Addiction: Increased Loneliness, Anxiety, and Depression. NeuroRegulation, 5(1), 3–3. https://doi.org/10.15540/nr.5.1.3
Perry, B. D. (2006a). Applying Principles of Neurodevelopment to Clinical Work with Maltreated and Traumatized Children: The Neurosequential Model of Therapeutics. In Working with traumatized youth in child welfare (pp. 27–52). The Guilford Press.
Perry, B. D. (2006b). Fear and learning: Trauma‐related factors in the adult education process. New Directions for Adult and Continuing Education, 2006(110), 21–27. https://doi.org/10.1002/ace.215
Perry, B. D. (2009). Examining Child Maltreatment Through a Neurodevelopmental Lens: Clinical Applications of the Neurosequential Model of Therapeutics. Journal of Loss and Trauma, 14(4), 240–255. https://doi.org/10.1080/15325020903004350
Perry, B. D. (2014). The Neurosequential Model of Therapeutics: Application of a developmentally sensitive and neurobiology-informed approach to clinical problem solving in maltreated children. In Infant and early childhood mental health: Core concepts and clinical practice (pp. 21–53). American Psychiatric Publishing, Inc.
Petrov, P., Manolova, V., & Vezenkov, S. (2025). Hidden Family Dynamics in a Case Study of a Child with Screen Addiction, Hyperactivity, and Language Deficits. Nootism, 1(1), 90–95. https://doi.org/10.64441/nootism.2NCSC.10
Petrova, S., Manolova, V., & Vezenkov, S. (2025). Reintroducing Screens: Severe Regression and Symptom Aggravation in Children with ASD/Screen Addiction. Nootism, 1(1), 59–65. https://doi.org/10.64441/nootism.2NCSC.5
Porges, S. W. (2003). Social engagement and attachment: A phylogenetic perspective. Annals of the New York Academy of Sciences, 1008, 31–47. https://doi.org/10.1196/annals.1301.004
Porges, S. W. (2007). The polyvagal perspective. Biological Psychology, 74(2), 116–143. https://doi.org/10.1016/j.biopsycho.2006.06.009
Porges, S. W. (2009). The polyvagal theory: New insights into adaptive reactions of the autonomic nervous system. Cleveland Clinic Journal of Medicine, 76(4 suppl 2), S86–S90. https://doi.org/10.3949/ccjm.76.s2.17
Porges, S. W. (2021). Polyvagal Theory: A biobehavioral journey to sociality. Comprehensive Psychoneuroendocrinology, 7, 100069. https://doi.org/10.1016/j.cpnec.2021.100069
Porges, S. W. (2023). The vagal paradox: A polyvagal solution. Comprehensive Psychoneuroendocrinology, 16, 100200. https://doi.org/10.1016/j.cpnec.2023.100200
Porges, S. W. (2025a). Deconstructing Autism Through the Lens of the Polyvagal Theory: A foreword to Understanding Autism edited by Drs. Papaneophytou and Das. In Understanding Autism (pp. xxiii–xxx). Elsevier. https://doi.org/10.1016/B978-0-443-27366-7.09998-3
Porges, S. W. (2025b). Polyvagal theory: A journey from physiological observation to neural innervation and clinical insight. Frontiers in Behavioral Neuroscience, 19, 1659083. https://doi.org/10.3389/fnbeh.2025.1659083
Raichle, M. E. (2015). The Brain’s Default Mode Network. Annual Review of Neuroscience, 38(Volume 38, 2015), 433–447. https://doi.org/10.1146/annurev-neuro-071013-014030
Rizzolatti, G., & Craighero, L. (2004). THE MIRROR-NEURON SYSTEM. Annual Review of Neuroscience, 27(Volume 27, 2004), 169–192. https://doi.org/10.1146/annurev.neuro.27.070203.144230
Rizzolatti, G., & Sinigaglia, C. (2016). The mirror mechanism: A basic principle of brain function. Nature Reviews. Neuroscience, 17(12), 757–765. https://doi.org/10.1038/nrn.2016.135
Schilbach, L., Timmermans, B., Reddy, V., Costall, A., Bente, G., Schlicht, T., & Vogeley, K. (2013). Toward a second-person neuroscience. Behavioral and Brain Sciences, 36(4), 393–414. https://doi.org/10.1017/S0140525X12000660
Selman, S. B., & Dilworth‐Bart, J. E. (2024). Routines and child development: A systematic review. Journal of Family Theory & Review, 16(2), 272–328. https://doi.org/10.1111/jftr.12549
Stefanova, M., Manolova, V., & Vezenkov, S. (2025). ADHD and Screen Addiction in Children Aged 3-9: Staged Recovery and Neurophysiological Markers. Nootism, 1(1), 66–73. https://doi.org/10.64441/nootism.2NCSC.6
Strouse, G. A., & Samson, J. E. (2021). Learning From Video: A Meta-Analysis of the Video Deficit in Children Ages 0 to 6 Years. Child Development, 92(1), e20–e38. https://doi.org/10.1111/cdev.13429
Sundqvist, A., Barr, R., Heimann, M., Birberg-Thornberg, U., & Koch, F.-S. (2024). A longitudinal study of the relationship between children’s exposure to screen media and vocabulary development. Acta Paediatrica, 113(3), 517–522. https://doi.org/10.1111/apa.17047
Swing, E. L., Gentile, D. A., Anderson, C. A., & Walsh, D. A. (2010). Television and Video Game Exposure and the Development of Attention Problems. Pediatrics, 126(2), 214–221. https://doi.org/10.1542/peds.2009-1508
Swingle, M. K. (2019). i-Minds - 2nd edition: How and Why Constant Connectivity is Rewiring Our Brains and What to Do About it. New Society Publishers.
Thayer, J. F., Hansen, A. L., Saus-Rose, E., & Johnsen, B. H. (2009). Heart Rate Variability, Prefrontal Neural Function, and Cognitive Performance: The Neurovisceral Integration Perspective on Self-regulation, Adaptation, and Health. Annals of Behavioral Medicine, 37(2), 141–153. https://doi.org/10.1007/s12160-009-9101-z
Uzundağ, B. A., Altundal, M. N., & Keşşafoğlu, D. (2022). Screen Media Exposure in Early Childhood and Its Relation to Children’s Self-Regulation. Human Behavior and Emerging Technologies, 2022, 1–34. https://doi.org/10.1155/2022/4490166
Uzundağ, B. A., Güven, İ. N., Sıvış, Ö., & Başpınar, G. (2026). Screen Media Exposure and Inhibitory Control: A Longitudinal Study From Infancy to Toddlerhood. Infancy: The Official Journal of the International Society on Infant Studies, 31(1), e70067. https://doi.org/10.1111/infa.70067
Van de Cruys, S., Evers, K., Van der Hallen, R., Van Eylen, L., Boets, B., de-Wit, L., & Wagemans, J. (2014). Precise minds in uncertain worlds: Predictive coding in autism. Psychological Review, 121(4), 649–675. https://doi.org/10.1037/a0037665
Vezenkov, S. (2016). COMPLEX PROGRAM FOR PREVENTION OF OCCUPATIONAL DEPRIVATION IN PERSONS WITH Irritable Bowel Syndrome (IBS) КОМПЛЕКСНА ПРОГРАМА ЗА ПРЕВЕНЦИЯ НА ДЕЙНОСТНИ ОГРАНИЧЕНИЯ ПРИ ЛИЦА СЪС СИНДРОМ НА РАЗДРАЗНЕНО ЧЕРВО. https://doi.org/10.13140/RG.2.2.10009.75365
Vezenkov, S. (2023). Биопсихосоциална хомеостаза # биофийдбек.
Vezenkov, S., & Iliev, D. (2019). Autonomous Neurotraining with Biofeedback Eliminates Completely Autonomous Chess Grandmaster Symptoms Occurring During Tournaments in Zeitnot (Case Study) (in bulgarian). https://doi.org/10.13140/RG.2.2.23177.39527
Vezenkov, S., & Manolova, V. (2024). Rethinking Autism: The Screen Addiction Paradigm. Conference Paper: BFE 22nd Meeting, 8–13. https://doi.org/10.13140/RG.2.2.27970.80328
Vezenkov, S., & Manolova, V. (2025a). A Three‑Stage Autonomic Biofeedback Program Improves IBS Symptoms and Quality of Life. Nootism, 1(5), 4–20. https://doi.org/10.64441/nootism.1.5.1
Vezenkov, S., & Manolova, V. (2025b). Neurobiology of Autism/Early Screen Addiction Recovery. Nootism, 1, 19–36. https://doi.org/10.64441/nootism.2NCSC.2
Vezenkov, S., & Manolova, V. (2025c). Screen Addiction – Biomarkers, Developmental Damage and Recovery. Nootism, 1(1), 6–18. https://doi.org/10.64441/nootism.2NCSC.1
Vezenkov, S., & Manolova, V. (2025d). Screen-Induced Pathological Eye-Covering Reflex in Children with Early Screen Addiction. Nootism, 1(3), 5–10. https://doi.org/10.64441/nootism.1.3.1
Vezenkov, S., & Manolova, V. (2025e). Screen-Induced Pathological Vestibular Reflex: A Specific Marker of Early Screen Addiction. Nootism, 1(2), 5–10. https://doi.org/10.64441/nootism.1.2.1
Vezenkov, S., & Manolova, V. (2025f). Sensory Disintegration versus Sensory Deprivation: Vestibular-Visual Dynamics and Shared Behavioral Phenotypes in ASD and Early Blindness. Nootism, 1(6), 4–12. https://doi.org/10.64441/nootism.1.6.1
Vezenkov, S., & Mitev, S. (2015). A modified brief biofeedback protocol improves the quality of life in a female patient with severe irritable bowel syndrome: A case report. https://doi.org/10.13140/RG.2.1.1159.1767
Volkow, N. D., Michaelides, M., & Baler, R. (2019). The Neuroscience of Drug Reward and Addiction. Physiological Reviews, 99(4), 2115–2140. https://doi.org/10.1152/physrev.00014.2018
Volkow, N. D., Wang, G.-J., Newcorn, J. H., Kollins, S. H., Wigal, T. L., Telang, F., Fowler, J. S., Goldstein, R. Z., Klein, N., Logan, J., Wong, C., & Swanson, J. M. (2011). Motivation deficit in ADHD is associated with dysfunction of the dopamine reward pathway. Molecular Psychiatry, 16(11), 1147–1154. https://doi.org/10.1038/mp.2010.97
Wylie, D. R., Gutiérrez-Ibáñez, C., Gaede, A. H., Altshuler, D. L., & Iwaniuk, A. N. (2018). Visual-Cerebellar Pathways and Their Roles in the Control of Avian Flight. Frontiers in Neuroscience, 12, 223. https://doi.org/10.3389/fnins.2018.00223
Zamfir, M. T. (n.d.). THE CONSUMPTION OF VIRTUAL ENVIRONMENT MORE THAN 4 HOURS/DAY, IN THE CHILDREN BETWEEN 0-3 YEARS OLD, CAN CAUSE A SYNDROME SIMILAR WITH THE AUTISM SPECTRUM DISORDER.
Zeanah, C. H., Gunnar, M. R., McCall, R. B., Kreppner, J. M., & Fox, N. A. (2011). Sensitive Periods. Monographs of the Society for Research in Child Development, 76(4), 147–162. https://doi.org/10.1111/j.1540-5834.2011.00631.x
Zhang, Z., Adamo, K. B., Ogden, N., Goldfield, G. S., Okely, A. D., Kuzik, N., Crozier, M., Hunter, S., Predy, M., & Carson, V. (2022). Associations between screen time and cognitive development in preschoolers. Paediatrics & Child Health, 27(2), 105–110. https://doi.org/10.1093/pch/pxab067
Zlatkova, K. (2025). Neurofeedback for Brain Dysregulation in Autism: QEEG and swLORETA Case Findings in the Context of Frequent Screen Exposure. Nootism, 1(4), 55–68. https://doi.org/10.64441/nootism.1.4.4